

Photoacoustic and fluorescence image-guided surgery using a multifunctional targeted nanoprobe
- PMID: 24554061
- PMCID: PMC4908963
- DOI: 10.1245/s10434-014-3541-9
Photoacoustic and fluorescence image-guided surgery using a multifunctional targeted nanoprobe
Abstract
Purpose: A complete surgical excision with negative tumor margins is the single most important factor in the prediction of long-term survival for most cancer patients with solid tumors. We hypothesized that image-guided surgery using nanoparticle-enhanced photoacoustic and fluorescence imaging could significantly reduce the rate of local recurrence.
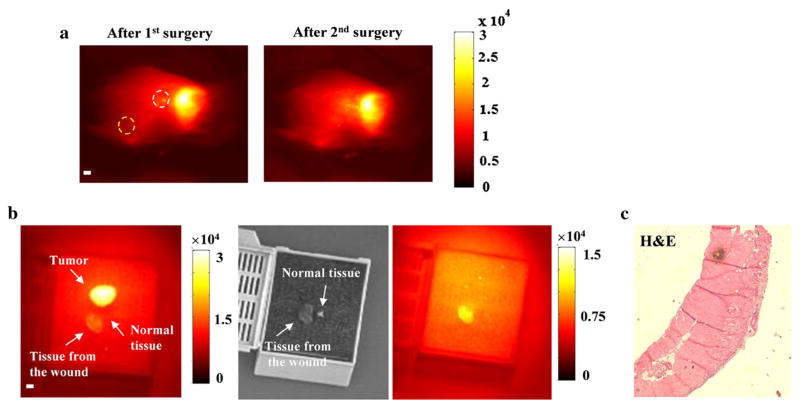
Methods: A murine model of invasive mammary carcinoma was utilized. Three experimental groups were included: (1) control; (2) tumor-bearing mice injected with non-targeted nanoprobe; and (3) tumor-bearing mice injected with targeted nanoprobe. The surgeon removed the primary tumor following the guidance of photoacoustic imaging (PAI), then inspected the surgical wound and removed the suspicious tissue using intraoperative near-infrared (NIR) fluorescence imaging. The mice were followed with bioluminescence imaging weekly to quantify local recurrence.
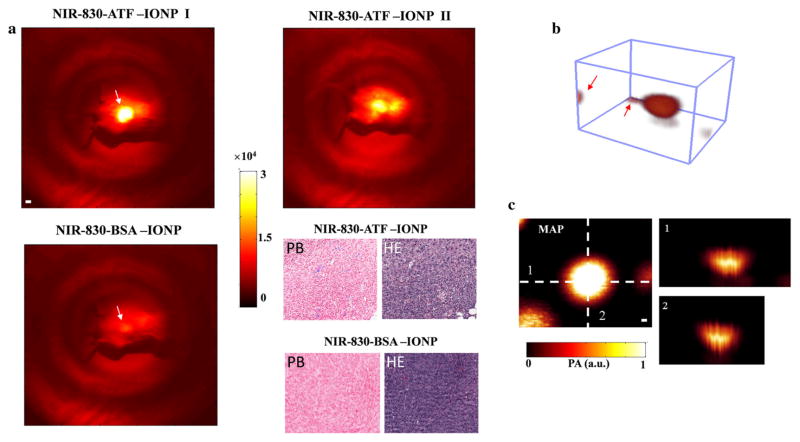
Results: Nanoprobe-enhanced photoacoustic contrast enabled PAI to map the volumetric tumor margins up to a depth of 31 mm. The targeted nanoparticles provided significantly greater enhancement than non-targeted nanoparticles. Seven mice in the group injected with the targeted nanoprobes underwent additional resections based upon NIR fluorescence imaging. Pathological analysis confirmed residual cancer cells in the re-resected specimens in 5/7 mice. Image-guided resection resulted in a significant reduction in local recurrence; 8.7 and 33.3 % of the mice in the targeted and control groups suffered recurrence, respectively.
Conclusions: These results suggest that photoacoustic and NIR intraoperative imaging can effectively assist a surgeon to locate primary tumors and to identify residual disease in real-time. This technology has promise to overcome current clinical challenges that result in the need for second surgical procedures.
Conflict of interest statement
Figures

Similar articles
-
An Innovation for Treating Orthotopic Pancreatic Cancer by Preoperative Screening and Imaging-Guided Surgery.Mol Imaging Biol. 2019 Feb;21(1):67-77. doi: 10.1007/s11307-018-1209-8. Mol Imaging Biol. 2019. PMID: 29858735
-
A multifunctional targeted nanoprobe with high NIR-II PAI/MRI performance for precise theranostics of orthotopic early-stage hepatocellular carcinoma.J Mater Chem B. 2021 Nov 3;9(42):8779-8792. doi: 10.1039/d1tb01729b. J Mater Chem B. 2021. PMID: 34635903
-
Synthesis, Characterization, and Biomedical Applications of a Targeted Dual-Modal Near-Infrared-II Fluorescence and Photoacoustic Imaging Nanoprobe.ACS Nano. 2017 Dec 26;11(12):12276-12291. doi: 10.1021/acsnano.7b05966. Epub 2017 Dec 11. ACS Nano. 2017. PMID: 29202225
-
Optical innovations in surgery.Br J Surg. 2015 Jan;102(2):e56-72. doi: 10.1002/bjs.9713. Br J Surg. 2015. PMID: 25627136 Review.
-
Near-IR emissive rare-earth nanoparticles for guided surgery.Theranostics. 2020 Feb 3;10(6):2631-2644. doi: 10.7150/thno.40808. eCollection 2020. Theranostics. 2020. PMID: 32194825 Free PMC article. Review.
Cited by
-
Photoacoustic-guided surgery from head to toe [Invited].Biomed Opt Express. 2021 Mar 16;12(4):2079-2117. doi: 10.1364/BOE.417984. eCollection 2021 Apr 1. Biomed Opt Express. 2021. PMID: 33996218 Free PMC article. Review.
-
Synthetic-aperture based photoacoustic re-beamforming (SPARE) approach using beamformed ultrasound data.Biomed Opt Express. 2016 Jul 19;7(8):3056-68. doi: 10.1364/BOE.7.003056. eCollection 2016 Aug 1. Biomed Opt Express. 2016. PMID: 27570697 Free PMC article.
-
Indocyanine Green Loaded Reduced Graphene Oxide for In Vivo Photoacoustic/Fluorescence Dual-Modality Tumor Imaging.Nanoscale Res Lett. 2016 Dec;11(1):85. doi: 10.1186/s11671-016-1288-x. Epub 2016 Feb 12. Nanoscale Res Lett. 2016. PMID: 26868422 Free PMC article.
-
Promotion of initial anti-tumor effect via polydopamine modified doxorubicin-loaded electrospun fibrous membranes.Int J Clin Exp Pathol. 2014 Aug 15;7(9):5436-49. eCollection 2014. Int J Clin Exp Pathol. 2014. PMID: 25337186 Free PMC article.
-
Photoacoustic image-guided interventions.Exp Biol Med (Maywood). 2020 Feb;245(4):330-341. doi: 10.1177/1535370219889323. Epub 2019 Nov 20. Exp Biol Med (Maywood). 2020. PMID: 31747782 Free PMC article. Review.
References
-
- Assersohn L, Powles TJ, Ashley S, et al. Local relapse in primary breast cancer patients with unexcised positive surgical margins after lumpectomy, radiotherapy and chemoendocrine therapy. Ann Oncol. 1999;10(12):1451–5. - PubMed
-
- Balch GC, Mithani SK, Simpson JF, Kelley MC. Accuracy of intraoperative gross examination of surgical margin status in women undergoing partial mastectomy for breast malignancy. Am Surg. 2005;71(1):22–7. - PubMed
-
- Sigal-Zafrani B, Lewis JS, Clough KB, et al. Histological margin assessment for breast ductal carcinoma in situ: precision and implications. Mod Pathol. 2004;17(1):81–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
