

Delayed surgical debridement in pediatric open fractures: a systematic review and meta-analysis
- PMID: 24554129
- PMCID: PMC3965772
- DOI: 10.1007/s11832-014-0567-2
Delayed surgical debridement in pediatric open fractures: a systematic review and meta-analysis
Abstract
Purpose: Open fractures are considered orthopedic emergencies that are traditionally treated with surgical debridement within 6 h of injury to prevent infection. However, this proclaimed "6-h rule" is arbitrary and not based on rigorous scientific evidence. The aim of our study was to systematically review the literature that compares late (>6 h from the time of injury) to early (<6 h from the time of injury) surgical debridement of pediatric open fractures.
Methods: We searched several databases from 1946 to 2013 for any observational or experimental studies that evaluated late and early surgical debridement of pediatric open fractures. We performed a meta-analysis using a random effects model to pool odds ratios for a comparison of infection rates between children undergoing late versus early surgical debridement. We also investigated the infection rates in upper- and lower-limb pediatric open fractures. Descriptive, quantitative, and qualitative data were extracted.
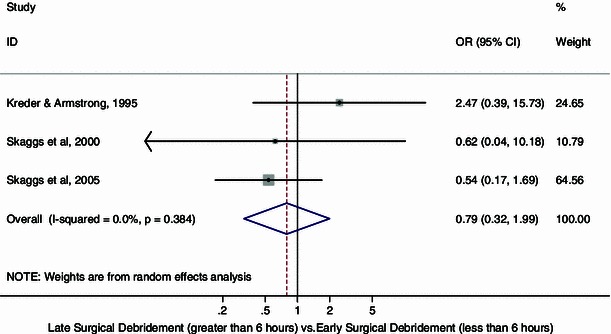
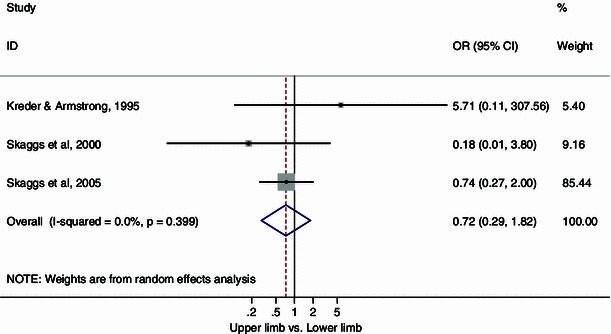
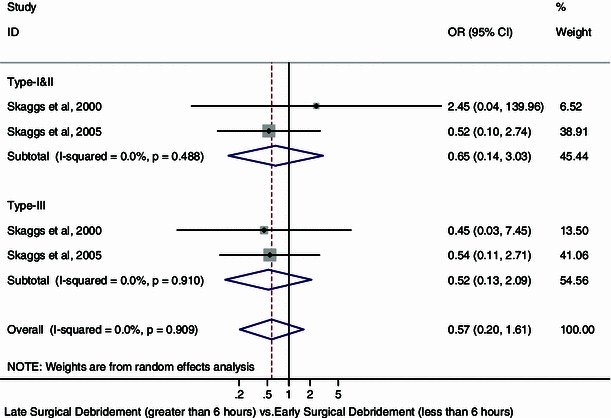
Results: Of the 12 articles identified, three studies (retrospective cohort studies) were eligible for the meta-analysis, encompassing a total of 714 open fractures. The pooled odds ratio (OR = 0.79) for infection between late and early surgical debridement was in favor of late surgical debridement but was not statistically significant (95 % CI 0.32, 1.99; p = 0.38, I (2) = 0 %). No significant difference in infection rate was detected between pediatric open fractures in the upper and lower limbs according to the time threshold in the included studies (OR = 0.72, 95 % CI 0.29, 1.82; p = 0.40, I (2) = 0 %).
Conclusions: The cumulative evidence does not, at present, indicate an association between late surgical debridement and higher infection rates in pediatric open fractures. However, initial expedient surgical debridement of open fractures in children should always remain the rule. Thus, multi-center randomized controlled trials or prospective cohort studies will be able to answer this question with more certainty and a higher level of evidence.
Level of evidence: Level III.
Figures
References
-
- Friedrich PL. Die aseptische Versorgung frischer Wunden. Arch Klin Chir. 1898;57:288–310.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
