

Diagnostic accuracy of maternal anthropometric measurements as predictors for dystocia in nulliparous women
- PMID: 24554954
- PMCID: PMC3917179
Diagnostic accuracy of maternal anthropometric measurements as predictors for dystocia in nulliparous women
Abstract
Background: Dystocia is one of the important causes of maternal morbidity and mortality in low-income countries. This study was aimed to determine the diagnostic accuracy of maternal anthropometric measurements as predictors for dystocia in nulliparous women.
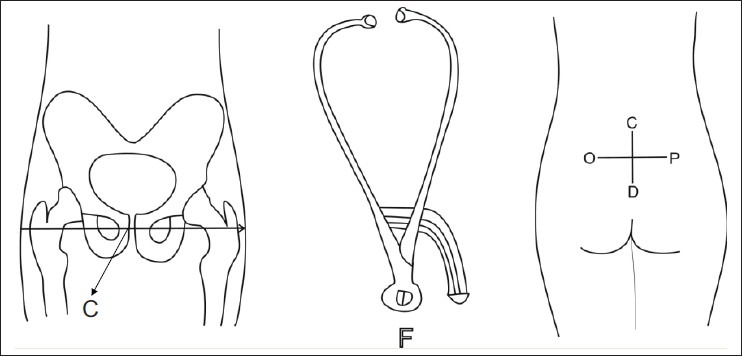
Materials and methods: This prospective cohort study was conducted on 447 nulliparous women who referred to Omolbanin hospital. Several maternal anthropometric measurements such as height, transverse and vertical diameters of Michaelis sacral rhomboid area, foot length, head circumference, vertebral and lower limb length, symphysio-fundal height, and abdominal girth were taken in cervical dilatation ≤ 5 cm. Labor progression was controlled by a researcher blind to these measurements. After delivery, the accuracy of individual and combined measurements in prediction of dystocia was analyzed. Dystocia was defined as cesarean section and vacuum or forceps delivery for abnormal progress of labor (cervical dilatation less than 1 cm/h in the active phase for 2 h, and during the second stage, beyond 2 h or fetal head descend less than 1 cm/h).
Results: Among the different anthropometric measurements, transverse diameter of the Michaelis sacral rhomboid area ≤9.6 cm, maternal height ≤ 155 cm, height to symphysio-fundal height ratio ≤4.7, lower limb length ≤78 cm, and head circumference to height ratio ≥ 35.05 with accuracy of 81.2%, 68.2%, 65.5%, 63.3%, and 61.5%, respectively, were better predictors. The best predictor was obtained by combination of maternal height ≤155 cm or the transverse diameter of the Michaelis sacral rhomboid area ≤9.6 cm and Johnson's formula estimated fetal weight ≥3255 g, with an accuracy of 90.5%, sensitivity of 70%, and specificity of 93.7%.
Conclusions: Combination of other anthropometric measurements and estimated fetal weight with maternal height in comparison to maternal height alone leads to a better predictor for dystocia.
Keywords: Anthropometric measurements; Iran; cephalopelvic disproportion; dystocia.
Conflict of interest statement
Figures
Similar articles
-
The diagnostic accuracy of external pelvimetry and maternal height to predict dystocia in nulliparous women: a study in Cameroon.BJOG. 2007 May;114(5):630-5. doi: 10.1111/j.1471-0528.2007.01294.x. BJOG. 2007. PMID: 17439570
-
Risk factors of dystocia in nulliparous women.Iran J Med Sci. 2014 May;39(3):254-60. Iran J Med Sci. 2014. PMID: 24850982 Free PMC article.
-
Maternal height and external pelvimetry to predict cephalopelvic disproportion in nulliparous African women: a cohort study.BJOG. 2000 Aug;107(8):947-52. doi: 10.1111/j.1471-0528.2000.tb10394.x. BJOG. 2000. PMID: 10955423
-
Labor Dystocia in Nulliparous Women.Am Fam Physician. 2021 Jan 15;103(2):90-96. Am Fam Physician. 2021. PMID: 33448772 Review.
-
[In case of fetal macrosomia, the best strategy is the induction of labor at 38 weeks of gestation].J Gynecol Obstet Biol Reprod (Paris). 2016 Nov;45(9):1037-1044. doi: 10.1016/j.jgyn.2016.09.001. Epub 2016 Oct 19. J Gynecol Obstet Biol Reprod (Paris). 2016. PMID: 27771202 Review. French.
Cited by
-
Can the Dynamic External Pelvimetry Test in Late Pregnancy Reveal Obstructed and Prolonged Labor? Results From a Pilot Study.Cureus. 2021 Dec 21;13(12):e20566. doi: 10.7759/cureus.20566. eCollection 2021 Dec. Cureus. 2021. PMID: 35103145 Free PMC article.
-
Inconsistent definitions of prolonged labor in international literature: a scoping review.AJOG Glob Rep. 2024 Jun 5;4(3):100360. doi: 10.1016/j.xagr.2024.100360. eCollection 2024 Aug. AJOG Glob Rep. 2024. PMID: 39040660 Free PMC article.
References
-
- Hofmery G. Obstructed labour: Using better technologies to reduce mortality. Int J Gynaecol Obstet. 2004;1:S62–72. - PubMed
-
- Surapanthapisit P, Thitadilok W. Risk factors of caesarean section due to cephalopelvic disproportion. J Med Assoc Thai. 2006;89:S105–11. - PubMed
-
- Liselele HB, Tshibangu CK, Meuris S. Association between External Pelvimetry and Vertex Delivery Complications in African Women. Acta Obstet Gynecol Scand. 2000;79:673–8. - PubMed
-
- Gregory KD, Niebyl JR, Johnson TR. Preconception and prenatal care: Part of the continuum. In: Gabbe SG, editor. Gbbe: Obstetrics Normal and Problem Pregnancies. 5th ed. New York: Churchill Livingstone Publishers; 2008. p. 102.
-
- Neilson JP, Lavender T, Quenby S, Wray S. Obstructed labor. Br Med Bull. 2003;67:191–204. - PubMed
LinkOut - more resources
Full Text Sources