

Predictive role of renal resistive index for clinical outcome after revascularization in hypertensive patients with atherosclerotic renal artery stenosis: a monocentric observational study
- PMID: 24555729
- PMCID: PMC3937242
- DOI: 10.1186/1476-7120-12-9
Predictive role of renal resistive index for clinical outcome after revascularization in hypertensive patients with atherosclerotic renal artery stenosis: a monocentric observational study
Abstract
Background: The present study evaluated the predictive value of renal resistive index (RI) for renal function and blood pressure (BP) outcome in hypertensive patients with unilateral atherosclerotic renal artery stenosis submitted to successful revascularization.
Methods: In 158 hypertensive patients with atherosclerotic renal artery stenosis RI was acquired. Twelve months after revascularization, they were classified on the basis of renal function and BP outcome as benefit (BP < 140/90 mmHg or diastolic BP reduction > 15 mmHg with the same of reduced drugs; decrease in glomerular filtration rate > 20%), or failure.
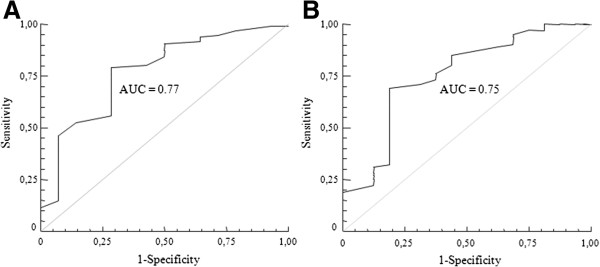
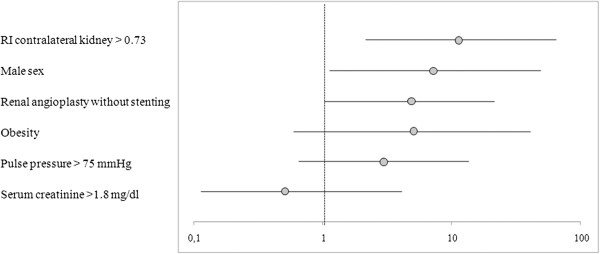
Results: Regarding renal function outcome, RI in the stenotic and in the contralateral kidney were significantly higher in patients with failure (n = 20) than in those with benefit (0.72 ± 0.11 vs 0.61 ± 0.11 and 0.76 ± 0.08 vs 0.66 ± 0.09, p < 0.05). Among different cutpoints generated, RI in the contralateral kidney >0.73 provided the largest area under the curve (0.77), and the highest sensitivity (80%) and specificity (72%). In the multivariate logistic regression analysis, RI in the contralateral kidney >0.73 was an independent predictor of a failure in renal function outcome.Regarding BP outcome, patients with no benefit from revascularization (n = 60) had similar RI in the stenotic and contralateral kidney (p = ns), but presented higher pulse pressure, albuminuria and hypertension duration in comparison to patients with improved BP control.
Conclusions: RI in the contralateral kidney is an independent predictor of renal function outcome after successful revascularization in hypertensive patients with unilateral atherosclerotic renal artery stenosis, whereas it is not able to predict blood pressure outcome.
Figures
References
-
- Rosenfield KA, Sacks D, Stanley JC, Taylor LM Jr, White CJ, White J, White RA, Antman EM, Smith SC Jr, Adams CD, Anderson JL, Faxon DP, Fuster V, Gibbons RJ, Hunt SA, Jacobs AK, Nishimura R, Ornato JP, Page RL, Riegel B. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation. 2006;113(11):e463–e654. - PubMed
-
- van Jaarsveld BC, Krijnen P, Pieterman H, Derkx FH, Deinum J, Postma CT, Dees A, Woittiez AJ, Bartelink AK, Man in’t Veld AJ, Schalekamp MA. The effect of balloon angioplasty on hypertension in atherosclerotic renal-artery stenosis. Dutch Renal Artery Stenosis Intervention Cooperative Study Group. N Engl J Med. 2000;342(14):1007–1014. doi: 10.1056/NEJM200004063421403. - DOI - PubMed
-
- Wheatley K, Ives N, Gray R, Kalra PA, Moss JG, Baigent C, Carr S, Chalmers N, Eadington D, Hamilton G, Lipkin G, Nicholson A, Scoble J. Revascularization versus medical therapy for renal-artery stenosis. N Engl J Med. 2009;361(20):1953–1962. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
