

Participation in cardiac rehabilitation, readmissions, and death after acute myocardial infarction
- PMID: 24556195
- PMCID: PMC4035431
- DOI: 10.1016/j.amjmed.2014.02.008
Participation in cardiac rehabilitation, readmissions, and death after acute myocardial infarction
Abstract
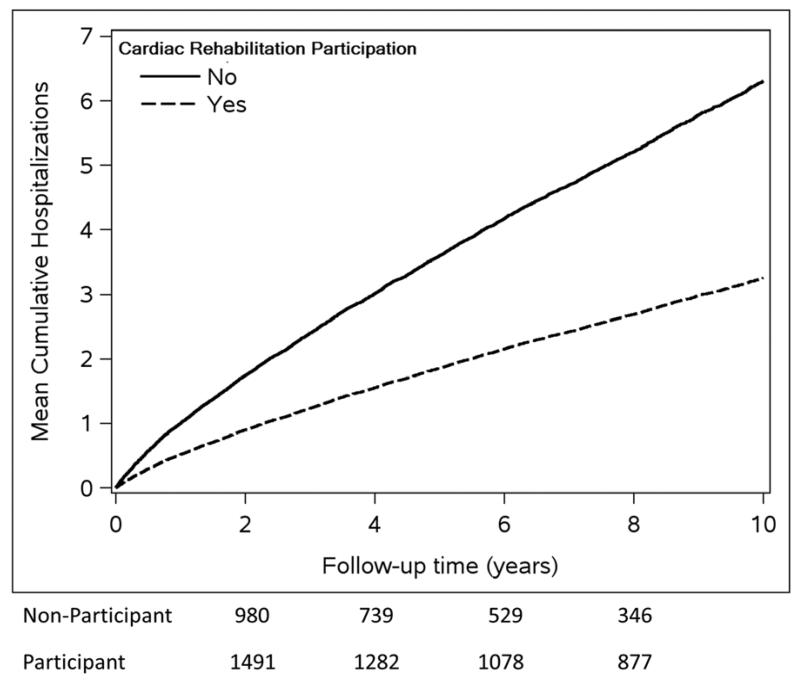
Background: Participation in cardiac rehabilitation has been shown to decrease mortality after acute myocardial infarction, but its impact on readmissions requires examination.
Methods: We conducted a population-based surveillance study of residents discharged from the hospital after their first-ever myocardial infarction in Olmsted County, Minnesota, from January 1, 1987, to September 30, 2010. Patients were followed up through December 31, 2010. Participation in cardiac rehabilitation after myocardial infarction was determined using billing data. We used a landmark analysis approach (cardiac rehabilitation participant vs not determined by attendance in at least 1 session of cardiac rehabilitation at 90 days post-myocardial infarction discharge) to compare readmission and mortality risk between cardiac rehabilitation participants and nonparticipants accounting for propensity to participate using inverse probability treatment weighting.
Results: Of 2991 patients with incident myocardial infarction, 1569 (52.5%) participated in cardiac rehabilitation after hospital discharge. The cardiac rehabilitation participation rate did not change during the study period, but increased in the elderly and decreased in men and younger patients. After adjustment, cardiac rehabilitation participants had lower all-cause readmission (hazard ratio [HR], 0.75; 95% confidence interval [CI], 0.65-0.87; P < .001), cardiovascular readmission (HR, 0.80; 95% CI, 0.65-0.99; P = .037), noncardiovascular readmission (HR, 0.72; 95% CI, 0.61-0.85; P < .001), and mortality (HR, 0.58; 95% CI, 0.49-0.68; P < .001) risk.
Conclusions: Cardiac rehabilitation participation is associated with a markedly reduced risk of readmission and death after incident myocardial infarction. Improving cardiac rehabilitation participation rates may have a large impact on post-myocardial infarction healthcare resource use and outcomes.
Keywords: Cardiac rehabilitation; Epidemiology; Myocardial infarction; Readmission; Survival.
Copyright © 2014 Elsevier Inc. All rights reserved.
Figures






References
-
- Go AS, Mozaffarian D, Roger VL, et al. Executive summary: heart disease and stroke statistics--2013 update: a report from the american heart association. Circulation. 2013;127:143–52. - PubMed
-
- Kostis WJ, Deng Y, Pantazopoulos JS, et al. Trends in mortality of acute myocardial infarction after discharge from the hospital. Circ Cardiovasc Qual Outcomes. 2010;3:581–9. - PubMed
-
-
Hospital Readmissions Reduction Program. Affordable Care Act., Subpart 1 of 42 CRT part 412. Sect. 1886(q) (2012).
-
-
- Witt BJ, Jacobsen SJ, Weston SA, et al. Cardiac rehabilitation after myocardial infarction in the community. J Am Coll Cardiol. 2004;44:988–96. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
