

Patient-reported and actionable safety events in CKD
- PMID: 24556352
- PMCID: PMC4073439
- DOI: 10.1681/ASN.2013090921
Patient-reported and actionable safety events in CKD
Abstract
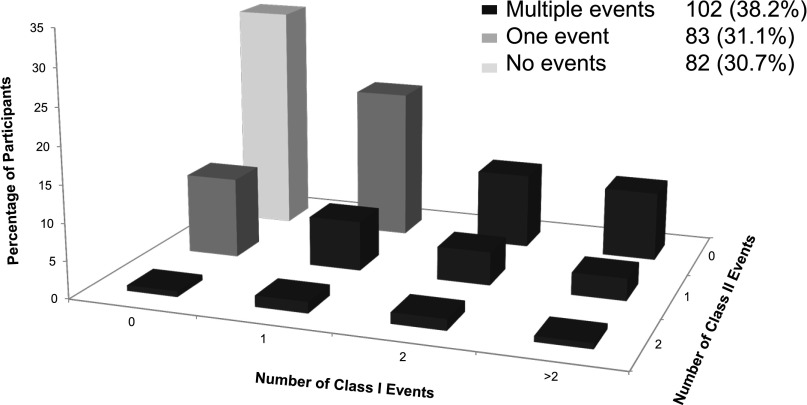
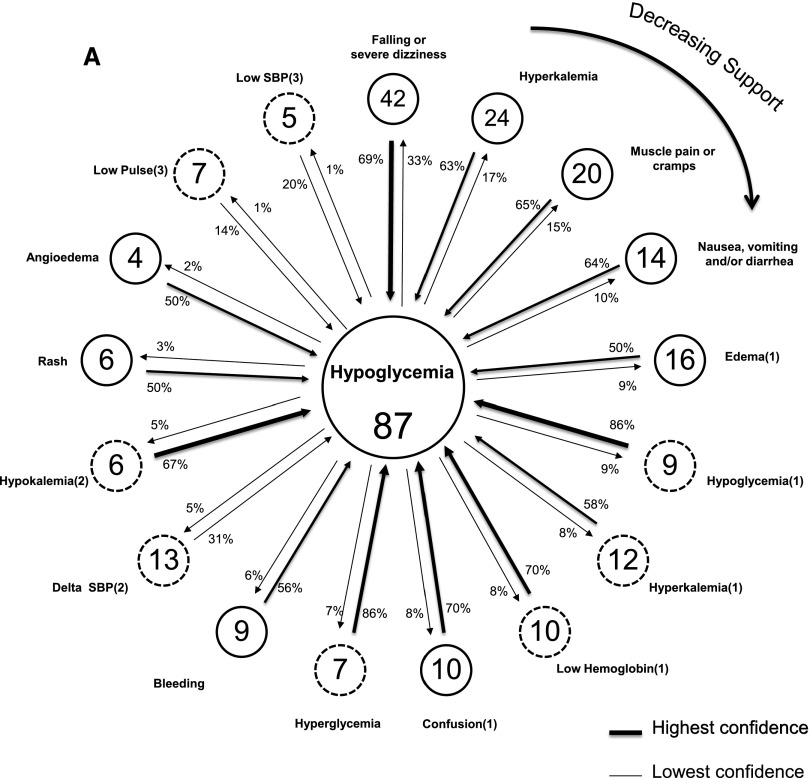
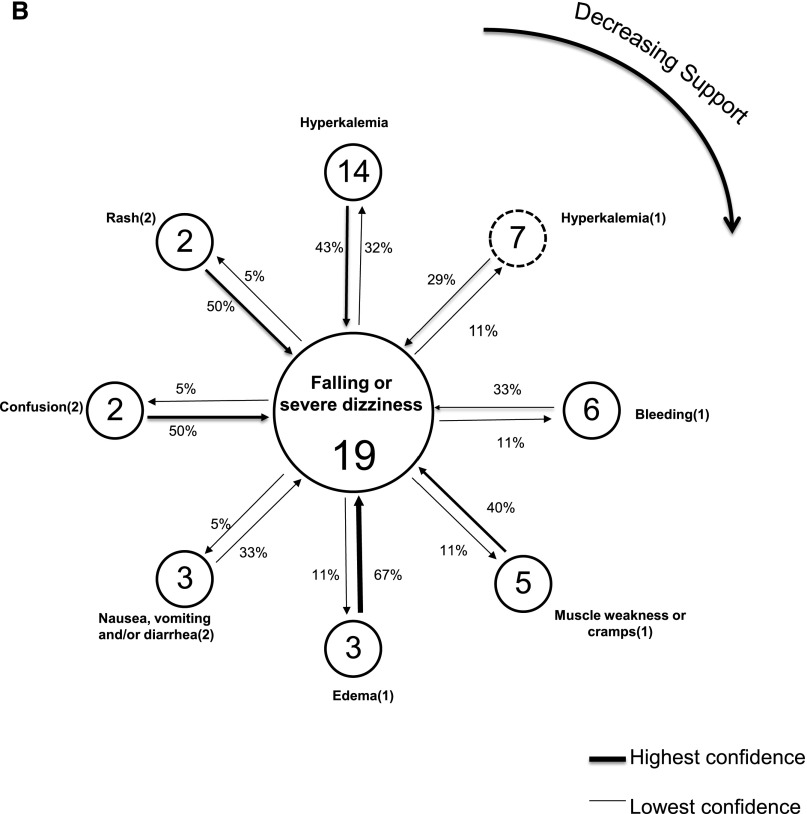
Patients with CKD are at high risk for adverse safety events because of the complexity of their care and impaired renal function. Using data from our observational study of predialysis patients with CKD enrolled in the Safe Kidney Care study, we estimated the baseline frequency of adverse safety events and determined to what extent these events co-occur. We examined patient-reported adverse safety incidents (class I) and actionable safety findings (class II), conditioned on participant use of drugs that might cause such an event, and we used association analysis as a data-mining technique to identify co-occurrences of these events. Of 267 participants, 185 (69.3%) had at least one class I or II event, 102 (38.2%) had more than one event, and 48 (18.0%) had at least one event from both classes. The adjusted conditional rates of class I and class II events ranged from 2.9 to 57.6 per 100 patients and from 2.2 to 8.3 per 100 patients, respectively. The most common conditional class I and II events were patient-reported hypoglycemia and hyperkalemia (serum potassium>5.5 mEq/L), respectively. Reporting of hypoglycemia (in patients with diabetes) and falling or severe dizziness (in patients without diabetes) were most frequently paired with other adverse safety events. We conclude that adverse safety events are common and varied in CKD, with frequent association between disparate events. Further work is needed to define the CKD "safety phenotype" and identify patients at highest risk for adverse safety events.
Keywords: chronic kidney disease; data mining; patient safety.
Copyright © 2014 by the American Society of Nephrology.
Figures
References
-
- Leape L, Berwick D, Clancy C, Conway J, Gluck P, Guest J, Lawrence D, Morath J, O’Leary D, O’Neill P, Pinakiewicz D, Isaac T, Lucian Leape Institute at the National Patient Safety Foundation : Transforming healthcare: A safety imperative. Qual Saf Health Care 18: 424–428, 2009 - PubMed
-
- Leape LL, Berwick DM: Five years after To Err Is Human: What have we learned? JAMA 293: 2384–2390, 2005 - PubMed
-
- McCannon CJ, Hackbarth AD, Griffin FA: Miles to go: An introduction to the 5 million lives campaign. Jt Comm J Qual Patient Saf 33: 477–484, 2007 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
