

A randomized controlled trial of mindfulness-based stress reduction to prevent flare-up in patients with inactive ulcerative colitis
- PMID: 24557009
- PMCID: PMC4059005
- DOI: 10.1159/000356316
A randomized controlled trial of mindfulness-based stress reduction to prevent flare-up in patients with inactive ulcerative colitis
Abstract
Background/aims: The primary therapeutic goals in ulcerative colitis (UC) are to maintain excellent quality of life (QOL) by treating flare-ups when they occur, and preventing flare-ups. Since stress can trigger UC flare-ups, we investigated the efficacy of mindfulness-based stress reduction (MBSR) to reduce flare-ups and improve QOL.
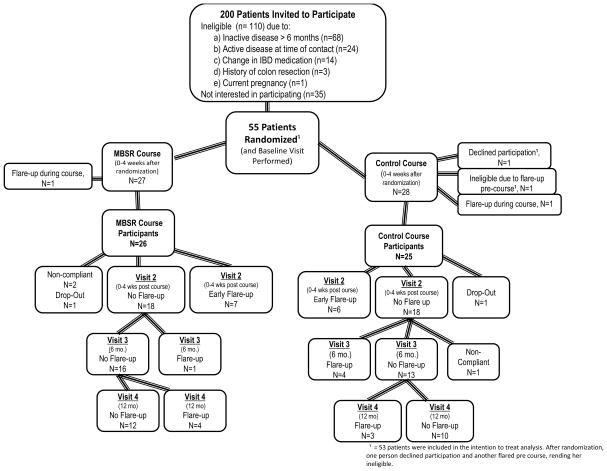
Methods: Patients with moderately severe UC, in remission, were randomized to MBSR or time/attention control. Primary outcome was disease status. Secondary outcomes were changes in markers of inflammation and disease activity, markers of stress and psychological assessments.
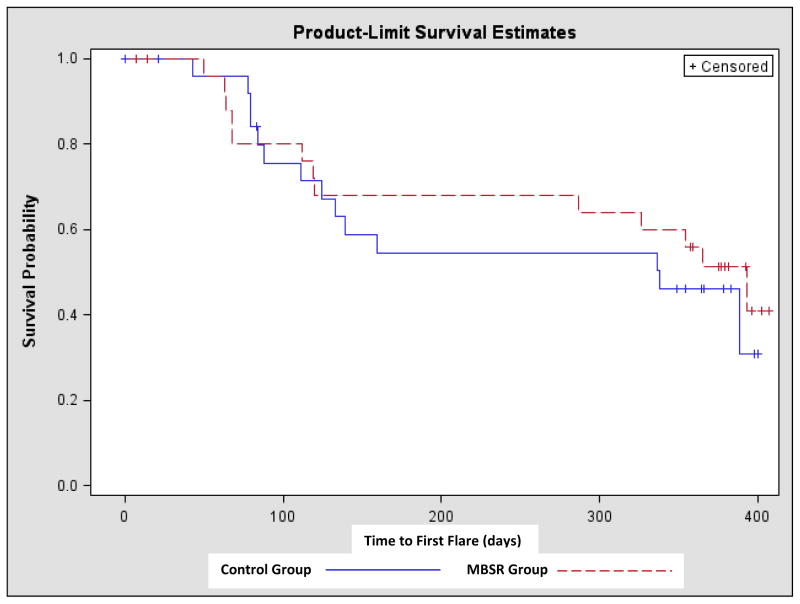
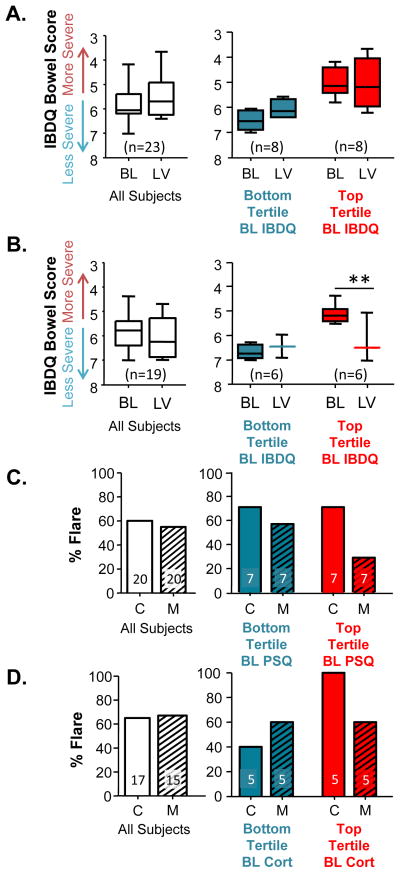
Results: 55 subjects were randomized. Absence of flares, time to flare and severity of flare over 1 year were similar between the two groups. However, post hoc analysis showed that MBSR decreased the proportion of participants with at least one flare-up among those with top tertile urinary cortisol and baseline perceived stress (30 vs. 70%; p < 0.001). MBSR patients who flared demonstrated significantly lower stress at the last visit compared to flared patients in the control group (p = 0.04). Furthermore, MBSR prevented a drop in the Inflammatory Bowel Disease Quality of Life Questionnaire during flare (p < 0.01).
Conclusion: MBSR did not affect the rate or severity of flare-ups in UC patients in remission. However, MBSR might be effective for those with high stress reactivity (high perceived stress and urinary cortisol) during remission. MBSR appears to improve QOL in UC patients by minimizing the negative impact of flare-ups on QOL. Further studies are needed to identify a subset of patients for whom MBSR could alter disease course.
Trial registration: ClinicalTrials.gov NCT00568256.
Figures
Comment in
-
It is about time - tailoring of an individualized multimodal treatment approach in ulcerative colitis.Digestion. 2014;89(2):139-41. doi: 10.1159/000357368. Epub 2014 Feb 14. Digestion. 2014. PMID: 24556964 No abstract available.
References
-
- Keighly MRB, Stockbrugger RW. Inflammatory bowel disease. Aliment Pharm Ther. 2003;18 (Suppl 3):66–70. - PubMed
-
- Navarro F, Hanauer S. Treatment of inflammatory bowel disease: Safety and tolerability issues. Am J Gastro. 2003;98:S18–23. - PubMed
-
- Kane SV, Cohen R, Aikens JE, et al. Predictors of non-compliance with mesalamine in quiescent ulcerative colitis. Am J Gastro. 2001;96:2929–32. - PubMed
-
- Levenstein S, Prantera C, Varvo V, et al. Stress and exacerbation in ulcerative colitis: A prospective study of patients enrolled in remission. Am J Gastroenterol. 2000;95:1213–9. - PubMed
-
- Maunder RG, Levenstein S. The role of stress in the development and clinical course of inflammatory bowel disease: epidemiological evidence. Curr Mol Med. 2008;8:247–52. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
