

A multicountry evaluation of careHPV testing, visual inspection with acetic acid, and papanicolaou testing for the detection of cervical cancer
- PMID: 24557438
- PMCID: PMC4047307
- DOI: 10.1097/IGC.0000000000000084
A multicountry evaluation of careHPV testing, visual inspection with acetic acid, and papanicolaou testing for the detection of cervical cancer
Abstract
Objective: This study evaluates the feasibility and performance of careHPV, a novel human papillomavirus (HPV) DNA test, when used for screening women for cervical cancer in low-resource settings.
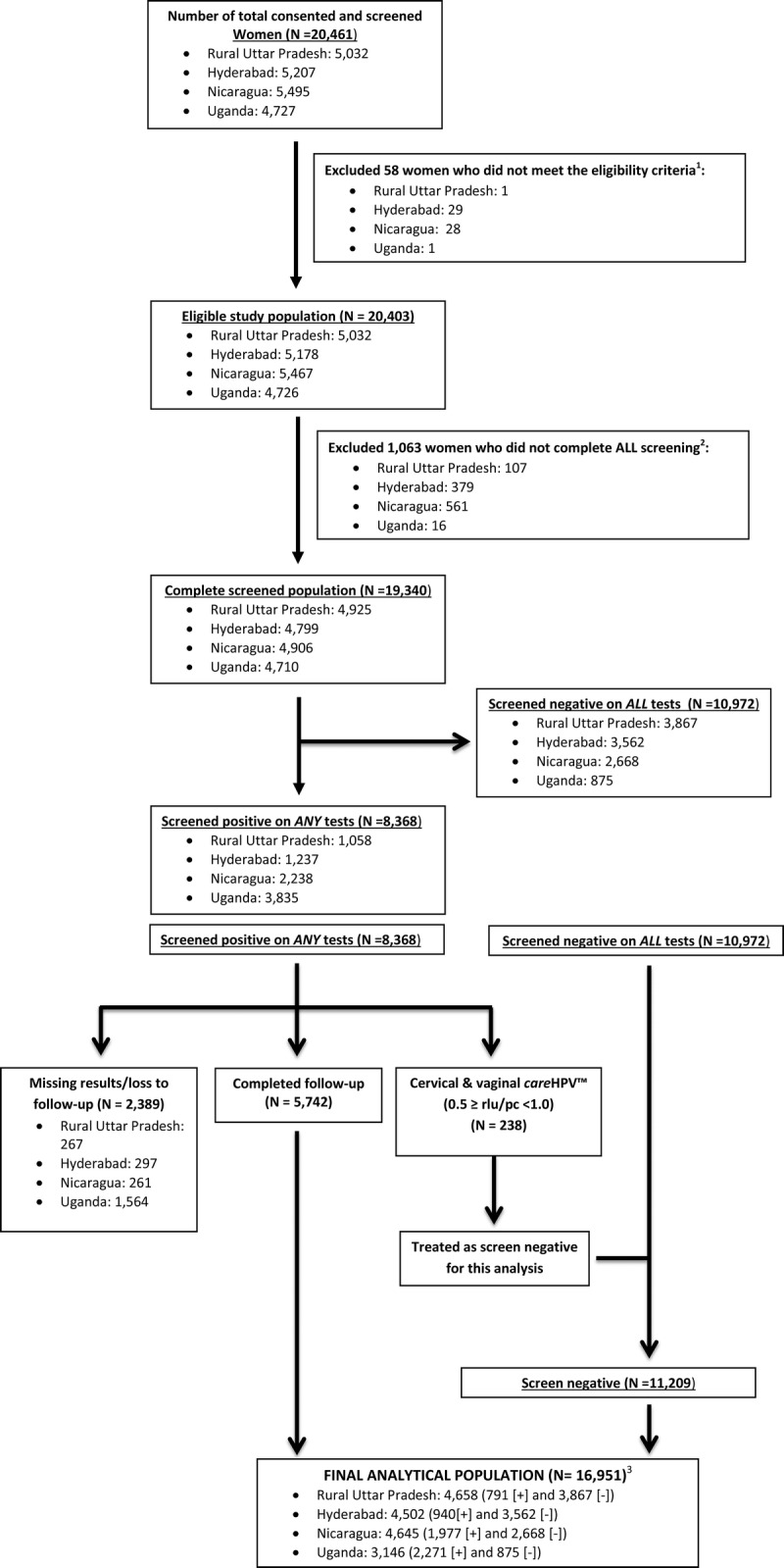
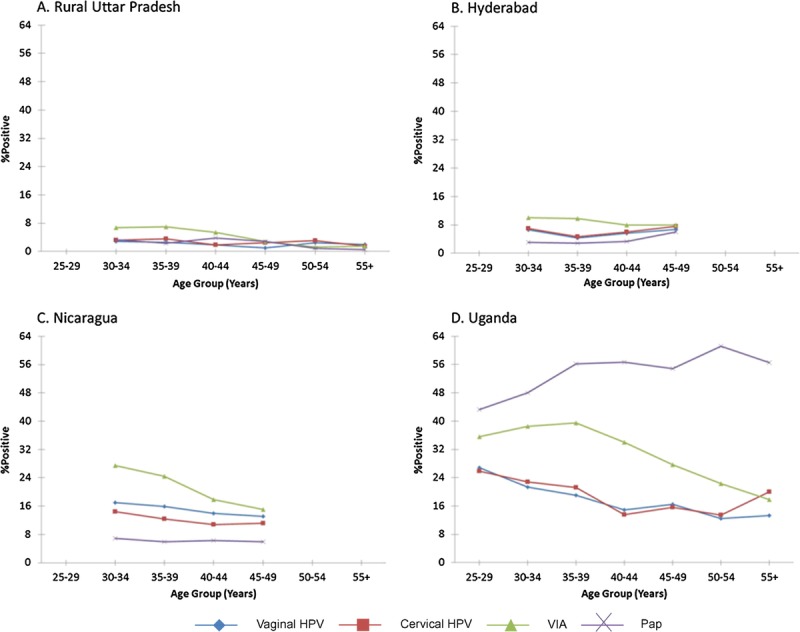
Methods and materials: Clinician-collected (cervical) and self-collected (vaginal) careHPV specimens, visual inspection with acetic acid (VIA), and Papanicolaou test were evaluated among 16,951 eligible women in India, Nicaragua, and Uganda. Women with positive screening results received colposcopy and histologic follow-up as indicated. The positivity of each screening method was calculated overall, by site, and age. In addition, the clinical performance of each screening test was determined for detection of cervical intraepithelial neoplasia (CIN) grade 2 (CIN2+) and CIN grade 3.
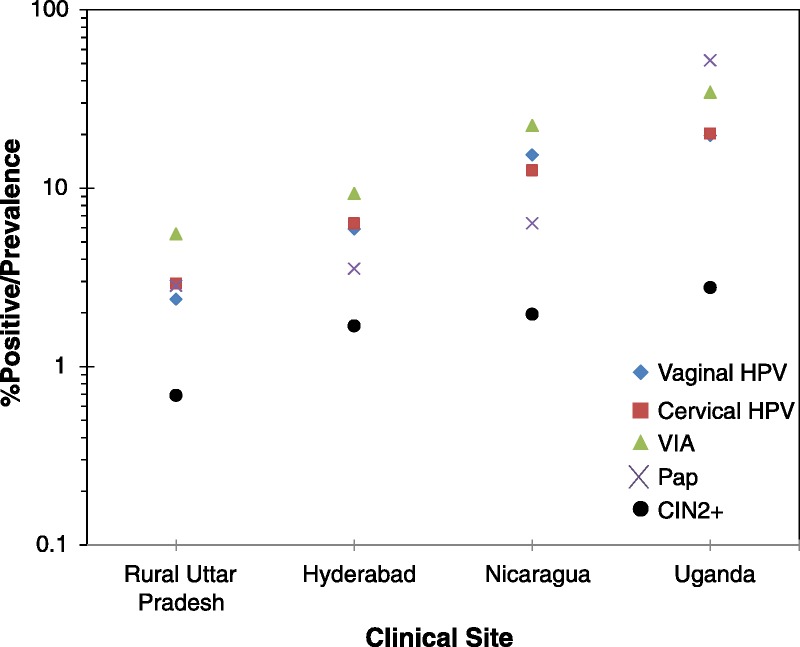
Results: Moderate or severe dysplasia or cancer (taken together as CIN2+) was diagnosed in 286 women. The positivity rate ranged between 2.4% to 19.6% for vaginal careHPV, 2.9% to 20.2% for cervical careHPV, 5.5% to 34.4% for VIA, and 2.8% to 51.8% for Papanicolaou test. Cervical careHPV was the most sensitive for CIN2+ (81.5%; 95% confidence interval [CI], 76.5-85.8) and CIN grade 3 (85.3%; 95% CI, 78.6-90.6) at all sites, followed by vaginal careHPV (69.6% and 71.3%, respectively). The sensitivity of VIA ranged from 21.9% to 73.6% and Papanicolaou test from 40.7% to 73.7%. The pooled specificities of cervical careHPV, vaginal careHPV, VIA, and Papanicolaou test were 91.6%, 90.6%, 84.2%, and 87.7%, respectively.
Conclusions: careHPV performed well in large multicountry demonstration studies conducted in resource-limited settings that have not previously been conducted this type of testing; its sensitivity using cervical samples or vaginal self-collected samples was better than VIA or Papanicolaou test. The feasibility of using careHPV in self-collected vaginal samples opens the possibility of increasing coverage and early detection in resource-constrained areas.
Conflict of interest statement
Philip E. Castle has received commercial HPV tests for research at a reduced or no cost from Roche, QIAGEN, Norchip, and MTM. He is a paid consultant for BD, GE Healthcare, Gen-Probe/Hologic, and Cepheid, and has received a speaker’s honorarium from Roche. He is a paid consultant for Immunexpress on sepsis diagnostics. He is compensated as a member of a Merck Data and Safety Monitoring Board for HPV vaccines. Jose Jeronimo was the director of the study and received all the tests used in the study as a donation from the manufacturing company (QIAGEN). Alice Lytwyn received grants for HPV research from McMaster University and payment from Bedard Lectureship for lecture on anal cancer. She also received payment for CD module on HPV from Merck Frosst and received travel and accommodations from the College of American Pathologists in related HVP work. The remaining authors delare no conflicts of interest.
Figures
References
-
- Ferlay J, Shin HR, Bray F, et al. Globocan 2008 v1.2, cancer incidence and mortality worldwide: IARC CancerBase No. 10. [Globocan Web site] 2010. Available at: http://globocan.iarc.fr/ Accessed April 2, 2013.
-
- International Agency for Research on Cancer. IARC Handbooks of Cancer Prevention: Cervix Cancer Screening. Lyon, France: IARC Press; 2005
-
- Muñoz N, Kjaer SK, Sigurdsson K, et al. Impact of human papillomavirus (HPV)-6/11/16/18 vaccine on all HPV-associated genital diseases in young women. J Natl Cancer Inst. 2010; 102: 325– 339 - PubMed
-
- Lehtinen M, Paavonen J, Wheeler CM, et al. Overall efficacy of HPV-16/18 AS04-adjuvanted vaccine against grade 3 or greater cervical intraepithelial neoplasia: 4-year end-of-study analysis of the randomised, double-blind PATRICIA trial. Lancet Oncol. 2012; 13: 89– 99 - PubMed
-
- Cuzick J, Clavel C, Petry KU, et al. Overview of the European and North American studies on HPV testing in primary cervical cancer screening. Int J Cancer. 2006; 119: 1095– 1101 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
