

Accelerated development of cervical spine instabilities in rheumatoid arthritis: a prospective minimum 5-year cohort study
- PMID: 24558457
- PMCID: PMC3928338
- DOI: 10.1371/journal.pone.0088970
Accelerated development of cervical spine instabilities in rheumatoid arthritis: a prospective minimum 5-year cohort study
Abstract
Objective: To clarify the incidence and predictive risk factors of cervical spine instabilities which may induce compression myelopathy in patients with rheumatoid arthritis (RA).
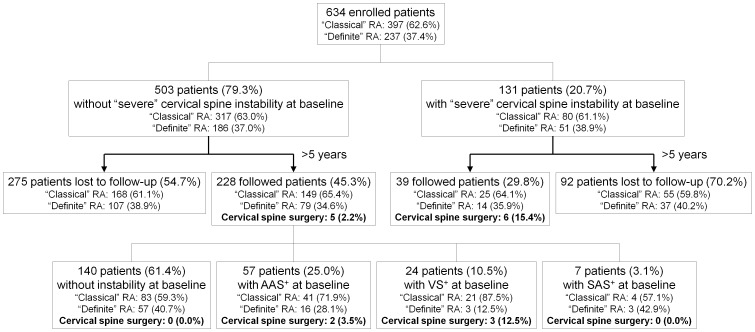
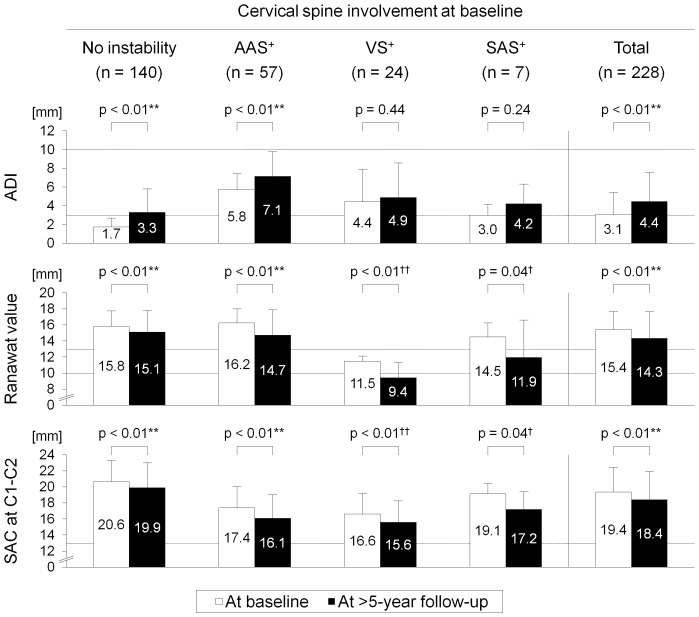
Methods: Three types of cervical spine instability were radiographically categorized into "moderate" and "severe" based on atlantoaxial subluxation (AAS: atlantodental interval >3 mm versus ≥10 mm), vertical subluxation (VS: Ranawat value <13 mm versus ≤10 mm), and subaxial subluxation (SAS: irreducible translation ≥2 mm versus ≥4 mm or at multiple). 228 "definite" or "classical" RA patients (140 without instability and 88 with "moderate" instability) were prospectively followed for >5 years. The endpoint incidence of "severe" instabilities and predictors for "severe" instability were determined.
Results: Patients with baseline "moderate" instability, including all sub-groups (AAS(+) [VS(-) SAS(-)], VS(+) [SAS(-) AAS(±)], and SAS(+) [AAS(±) VS(±)]), developed "severe" instabilities more frequently (33.3% with AAS(+), 75.0% with VS(+), and 42.9% with SAS(+)) than those initially without instability (12.9%; p<0.003, p<0.003, and p = 0.061, respectively). The incidence of cervical canal stenosis and/or basilar invagination was also higher in patients with initial instability (17.5% with AAS(+), 37.5% with VS(+), and 14.3% with SAS(+)) than in those without instability (7.1%; p = 0.028, p<0.003, and p = 0.427, respectively). Multivariable logistic regression analysis identified corticosteroid administration, Steinbrocker stage III or IV at baseline, mutilating changes at baseline, and the development of mutilans during the follow-up period correlated with the progression to "severe" instability (p<0.05).
Conclusions: This prospective cohort study demonstrates accelerated development of cervical spine involvement in RA patients with pre-existing instability--especially VS. Advanced peripheral erosiveness and concomitant corticosteroid treatment are indicators for poor prognosis of the cervical spine in RA.
Conflict of interest statement
Figures
Similar articles
-
Incidence and aggravation of cervical spine instabilities in rheumatoid arthritis: a prospective minimum 5-year follow-up study of patients initially without cervical involvement.Spine (Phila Pa 1976). 2012 Dec 15;37(26):2136-44. doi: 10.1097/BRS.0b013e31826def1c. Spine (Phila Pa 1976). 2012. PMID: 22895480
-
Predictive Risk Factors of Cervical Spine Instabilities in Rheumatoid Arthritis: A Prospective Multicenter Over 10-Year Cohort Study.Spine (Phila Pa 1976). 2017 Apr 15;42(8):556-564. doi: 10.1097/BRS.0000000000001853. Spine (Phila Pa 1976). 2017. PMID: 27525538
-
Progression of cervical spine instabilities in rheumatoid arthritis: a prospective cohort study of outpatients over 5 years.Spine (Phila Pa 1976). 2011 Apr 15;36(8):647-53. doi: 10.1097/BRS.0b013e3181da21c5. Spine (Phila Pa 1976). 2011. PMID: 21178849
-
Radiological evaluation of cervical spine involvement in rheumatoid arthritis.Neurosurg Focus. 2015 Apr;38(4):E4. doi: 10.3171/2015.1.FOCUS14664. Neurosurg Focus. 2015. PMID: 25828498 Review.
-
The Craniovertebral Junction in Rheumatoid Arthritis: State of the Art.Acta Neurochir Suppl. 2019;125:79-86. doi: 10.1007/978-3-319-62515-7_12. Acta Neurochir Suppl. 2019. PMID: 30610306 Review.
Cited by
-
Radiological assessment and surgical management of cervical spine involvement in patients with rheumatoid arthritis.Rheumatol Int. 2023 Feb;43(2):195-208. doi: 10.1007/s00296-022-05239-5. Epub 2022 Nov 15. Rheumatol Int. 2023. PMID: 36378323 Free PMC article. Review.
-
Prevalence of cervical spine instability among Rheumatoid Arthritis patients in South Iraq.J Clin Orthop Trauma. 2020 Sep-Oct;11(5):876-882. doi: 10.1016/j.jcot.2019.06.013. Epub 2019 Jun 14. J Clin Orthop Trauma. 2020. PMID: 32879574 Free PMC article.
-
Rheumatoid Arthritis Affecting the Upper Cervical Spine: Biomechanical Assessment of the Stabilizing Ligaments.Biomed Res Int. 2017;2017:6131703. doi: 10.1155/2017/6131703. Epub 2017 Oct 18. Biomed Res Int. 2017. PMID: 29181398 Free PMC article.
-
Prevalence and aggravation of cervical spine instabilities in rheumatoid arthritis during over 10 years: a prospective multicenter cohort study.Sci Rep. 2024 Nov 5;14(1):26821. doi: 10.1038/s41598-024-78429-9. Sci Rep. 2024. PMID: 39501065 Free PMC article.
-
[The rheumatic cervical spine].Z Rheumatol. 2017 Dec;76(10):838-847. doi: 10.1007/s00393-017-0388-z. Z Rheumatol. 2017. PMID: 28986633 Review. German.
References
-
- Alamanos Y, Drosos AA (2005) Epidemiology of adult rheumatoid arthritis. Autoimmun Rev 4: 130–136. - PubMed
-
- Martel W (1961) The occipito-atlanto-axial joints in rheumatoid arthritis and ankylosing spondylitis. Am J Roentgenol Radium Ther Nucl Med 86: 223–240. - PubMed
-
- Lourie H, Stewart WA (1961) Spontaneous atlantoaxial dislocation. A complication of rheumatoid disease. N Engl J Med 265: 677–681. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
