

Sciatic nerve injury related to hip replacement surgery: imaging detection by MR neurography despite susceptibility artifacts
- PMID: 24558483
- PMCID: PMC3928432
- DOI: 10.1371/journal.pone.0089154
Sciatic nerve injury related to hip replacement surgery: imaging detection by MR neurography despite susceptibility artifacts
Abstract
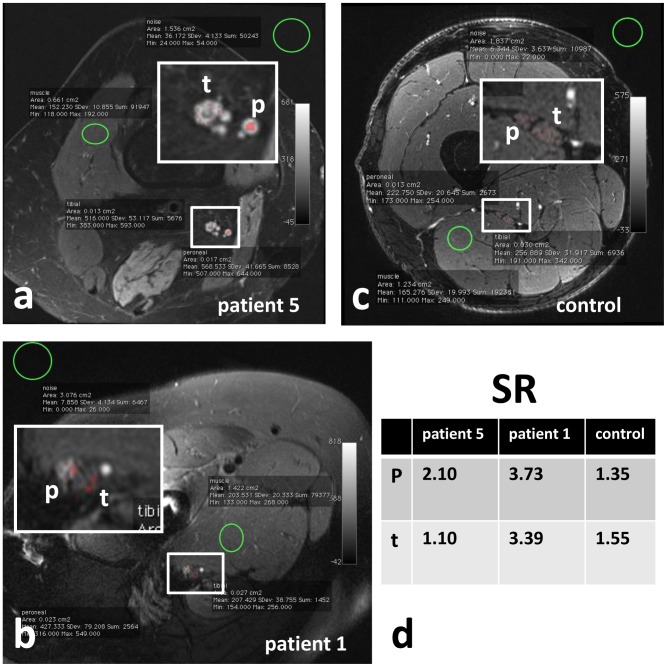
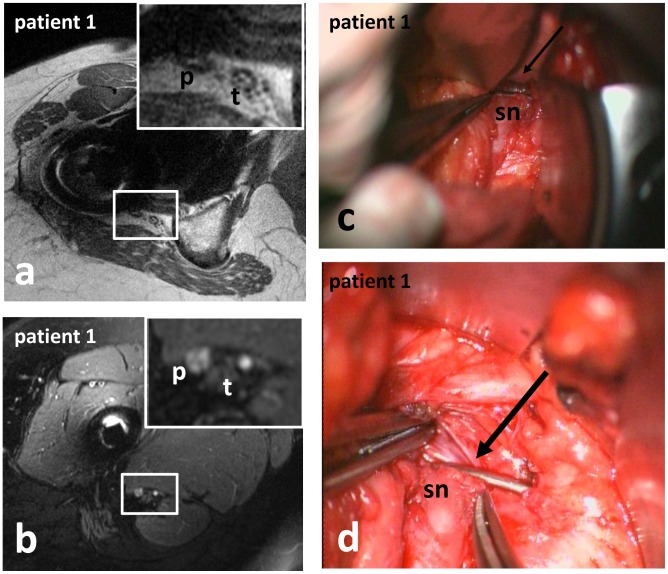
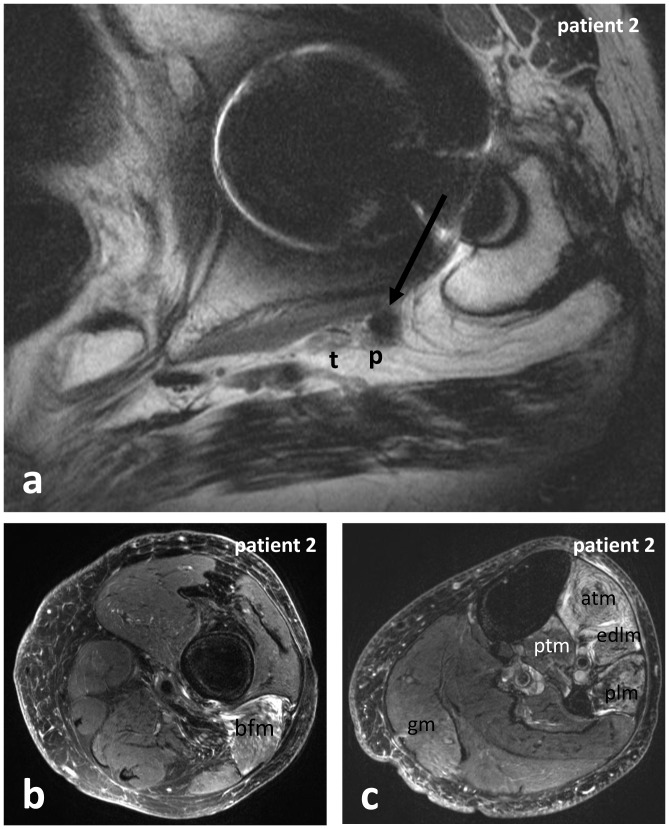
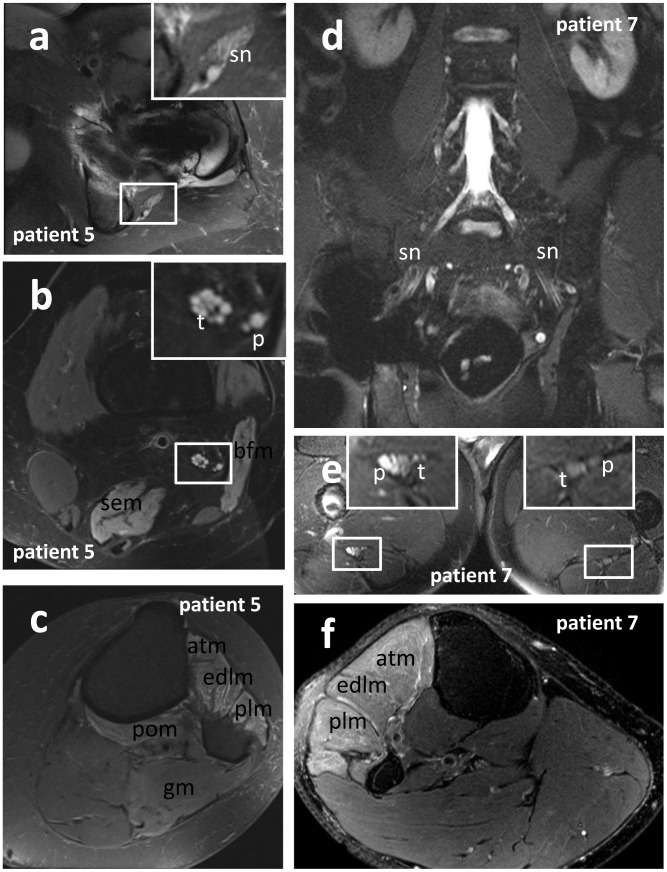
Sciatic nerve palsy related to hip replacement surgery (HRS) is among the most common causes of sciatic neuropathies. The sciatic nerve may be injured by various different periprocedural mechanisms. The precise localization and extension of the nerve lesion, the determination of nerve continuity, lesion severity, and fascicular lesion distribution are essential for assessing the potential of spontaneous recovery and thereby avoiding delayed or inappropriate therapy. Adequate therapy is in many cases limited to conservative management, but in certain cases early surgical exploration and release of the nerve is indicated. Nerve-conduction-studies and electromyography are essential in the diagnosis of nerve injuries. In postsurgical nerve injuries, additional diagnostic imaging is important as well, in particular to detect or rule out direct mechanical compromise. Especially in the presence of metallic implants, commonly applied diagnostic imaging tests generally fail to adequately visualize nervous tissue. MRI has been deemed problematic due to implant-related artifacts after HRS. In this study, we describe for the first time the spectrum of imaging findings of Magnetic Resonance neurography (MRN) employing pulse sequences relatively insensitive to susceptibility artifacts (susceptibility insensitive MRN, siMRN) in a series of 9 patients with HRS procedure related sciatic nerve palsy. We were able to determine the localization and fascicular distribution of the sciatic nerve lesion in all 9 patients, which clearly showed on imaging predominant involvement of the peroneal more than the tibial division of the sciatic nerve. In 2 patients siMRN revealed direct mechanical compromise of the nerve by surgical material, and in one of these cases indication for surgical release of the sciatic nerve was based on siMRN. Thus, in selected cases of HRS related neuropathies, especially when surgical exploration of the nerve is considered, siMRN, with its potential to largely overcome implant related artifacts, is a useful diagnostic addition to nerve-conduction-studies and electromyography.
Conflict of interest statement
Figures
Similar articles
-
Characterizing peroneal nerve injury clinicoradiological patterns with MRI in patients with sciatic neuropathy and foot drop after total hip replacement.J Neurosurg. 2023 Jun 23;139(6):1560-1567. doi: 10.3171/2023.5.JNS23173. Print 2023 Dec 1. J Neurosurg. 2023. PMID: 37382352
-
MR neurography of sciatic nerve injection injury.J Neurol. 2011 Jun;258(6):1120-5. doi: 10.1007/s00415-010-5895-7. Epub 2011 Jan 12. J Neurol. 2011. PMID: 21225276
-
Magnetic resonance neurography evaluation of chronic extraspinal sciatica after remote proximal hamstring injury: a preliminary retrospective analysis.J Neurosurg. 2014 Aug;121(2):408-14. doi: 10.3171/2014.4.JNS13940. Epub 2014 May 30. J Neurosurg. 2014. PMID: 24878283
-
Sciatic neuropathy.Neurol Clin. 1999 Aug;17(3):617-31, viii. doi: 10.1016/s0733-8619(05)70155-9. Neurol Clin. 1999. PMID: 10393756 Review.
-
Early surgical treatment protocol for sciatic nerve injury due to injection--a retrospective study.Br J Neurosurg. 2011 Aug;25(4):509-15. doi: 10.3109/02688697.2011.566380. Epub 2011 Apr 22. Br J Neurosurg. 2011. PMID: 21513449 Review.
Cited by
-
The Surgical Timing and Prognoses of Elderly Patients with Hip Fractures: A Retrospective Analysis.Clin Interv Aging. 2023 Jun 2;18:891-899. doi: 10.2147/CIA.S408903. eCollection 2023. Clin Interv Aging. 2023. PMID: 37287528 Free PMC article.
-
3D-engineering of Cellularized Conduits for Peripheral Nerve Regeneration.Sci Rep. 2016 Aug 30;6:32184. doi: 10.1038/srep32184. Sci Rep. 2016. PMID: 27572698 Free PMC article.
-
Distances between bony landmarks and adjacent nerves: anatomical factors that may influence retractor placement in total hip replacement surgery.J Orthop Surg Res. 2016 Mar 16;11:31. doi: 10.1186/s13018-016-0365-2. J Orthop Surg Res. 2016. PMID: 26984637 Free PMC article.
-
Type II sciatic nerve variant: an unexpected interventional hazard.Skeletal Radiol. 2017 Oct;46(10):1453-1458. doi: 10.1007/s00256-017-2712-8. Epub 2017 Jul 26. Skeletal Radiol. 2017. PMID: 28748363
-
Role of MR Neurography for Evaluation of the Lumbosacral Plexus: A Scoping Review.J Korean Soc Radiol. 2022 Nov;83(6):1273-1285. doi: 10.3348/jksr.2022.0001. Epub 2022 Nov 15. J Korean Soc Radiol. 2022. PMID: 36545407 Free PMC article.
References
-
- Zhan C, Kaczmarek R, Loyo-Berrios N, Sangl J, Bright RA (2007) Incidence and short-term outcomes of primary and revision hip replacement in the United States. J Bone Joint Surg Am 89: 526–533 89/3/526 [pii];10.2106/JBJS.F.00952 [doi]. - PubMed
-
- Farrell CM, Springer BD, Haidukewych GJ, Morrey BF (2005) Motor nerve palsy following primary total hip arthroplasty. J Bone Joint Surg Am 87: 2619–2625 87/12/2619 [pii];10.2106/JBJS.C.01564 [doi]. - PubMed
-
- Nercessian OA, Macaulay W, Stinchfield FE (1994) Peripheral neuropathies following total hip arthroplasty. J Arthroplasty 9: 645–651. 0883–5403(94)90119–8 [pii]. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
