

Changing trends of imaging in angle closure evaluation
- PMID: 24558589
- PMCID: PMC3914273
- DOI: 10.5402/2012/597124
Changing trends of imaging in angle closure evaluation
Abstract
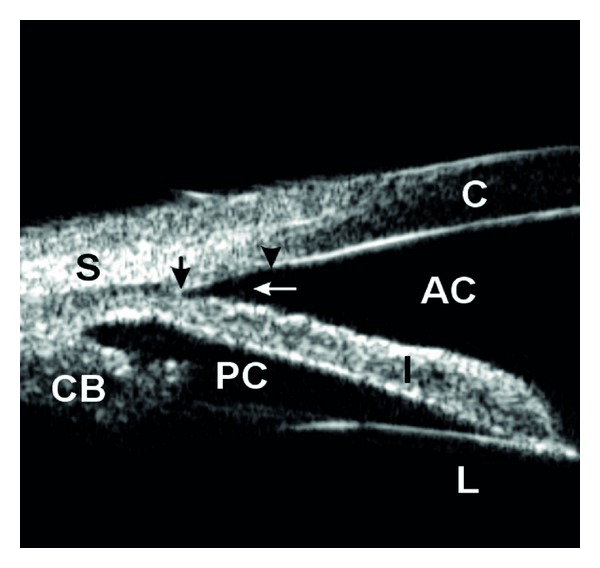
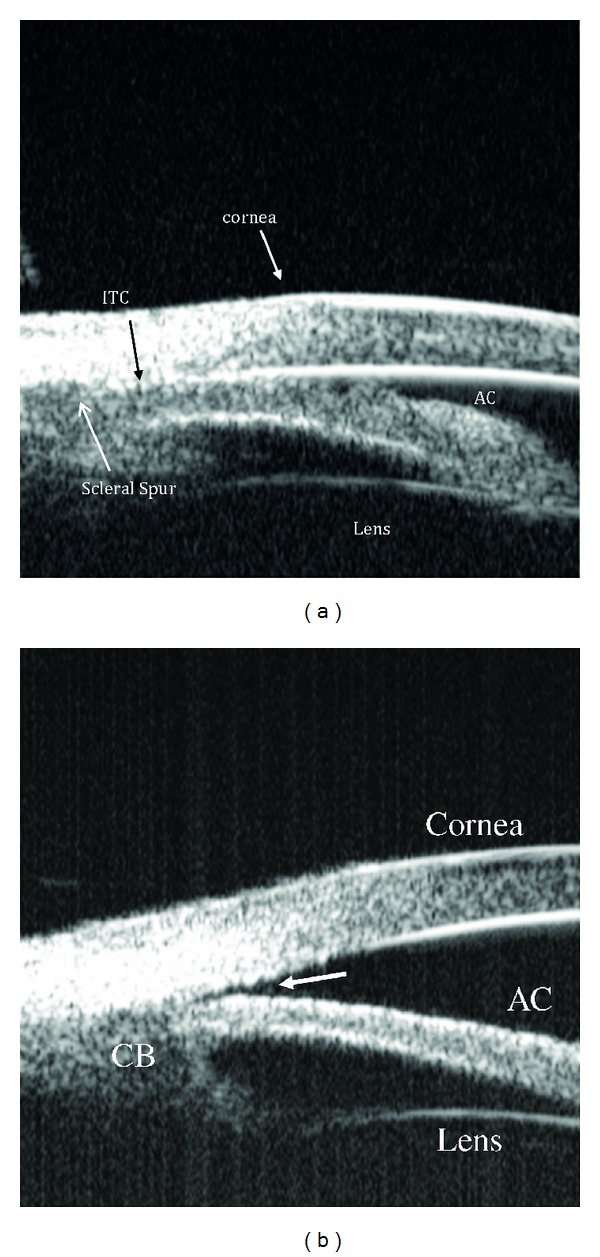
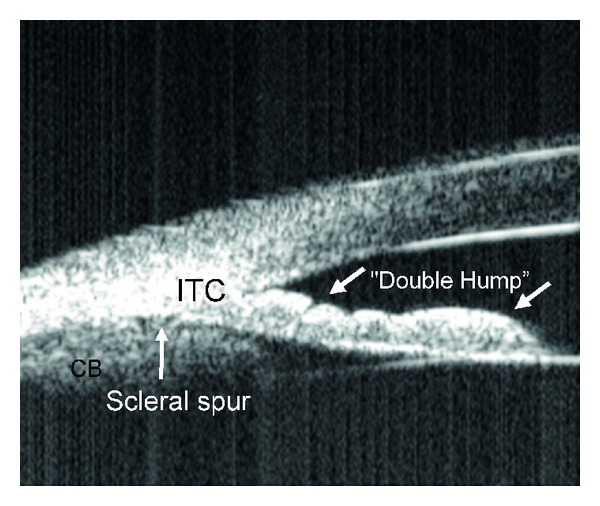
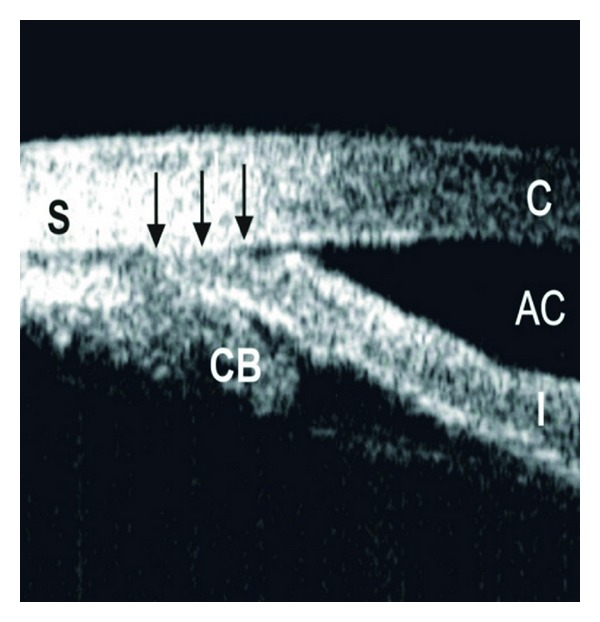
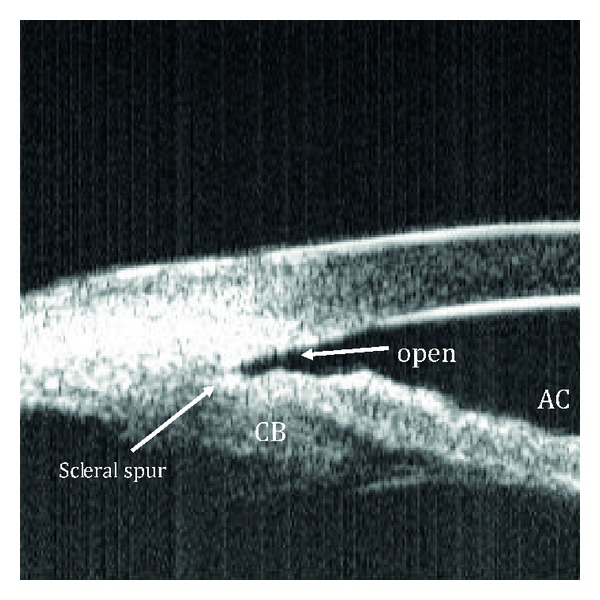
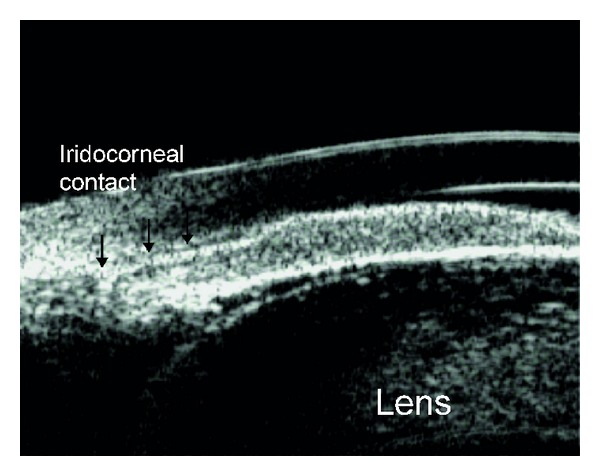
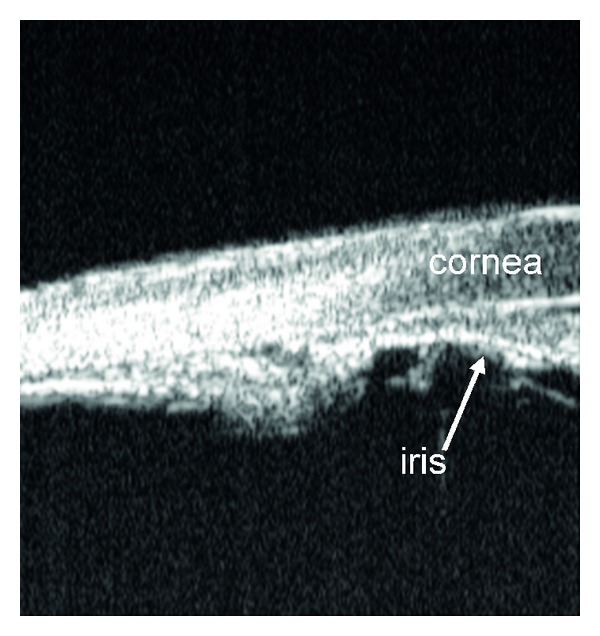
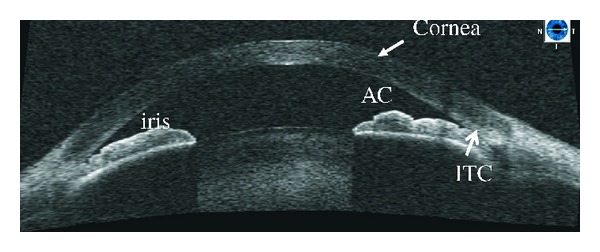
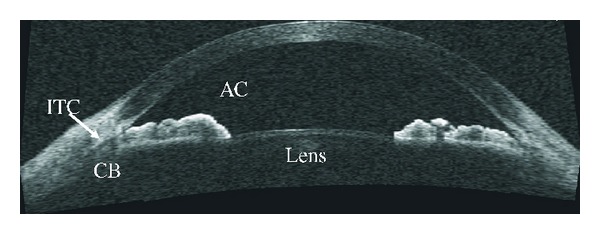
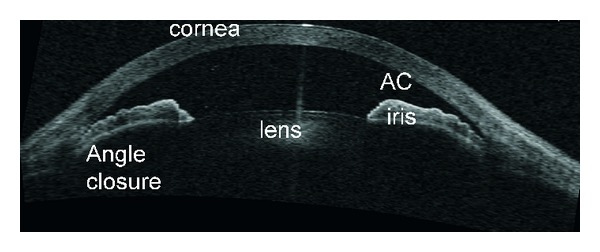
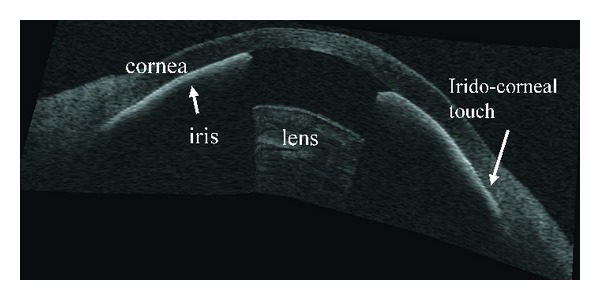
Primary angle closure glaucoma (PACG) is a significant cause of visual disability worldwide. It predominantly affects the Eastern and South Asian population of the world. Early detection of anatomically narrow angles is important, and the subsequent prevention of visual loss from PACG depends on an accurate assessment of the anterior chamber angle (ACA). Gonioscopy has given way to modern day imaging technologies such as ultrasound biomicroscopy (UBM) and more recently, anterior segment optical coherence tomography (AS-OCT). Ultrasound biomicroscopy provides objective, high-resolution images of anterior segment anatomy, including the cornea, iris, anterior chamber, anterior chamber angle, and ciliary body. Optical coherence tomography (OCT) is a noncontact optical signal acquisition and processing device that provides magnified, high-resolution cross-sectional images of ocular tissues. Recent technological advances towards three-dimensional visualization broadened the scope of AS-OCT in ophthalmologic evaluation. Optical coherence tomography systems use low-coherence, near-infrared light to provide detailed images of anterior segment structures at resolutions exceeding that of UBM. This paper summarizes the clinical application of UBM and OCT for assessment of anterior segment in glaucoma.
Figures
Similar articles
-
Anterior-segment imaging for assessment of glaucoma.Expert Rev Ophthalmol. 2010 Feb 1;5(1):59-74. doi: 10.1586/eop.09.61. Expert Rev Ophthalmol. 2010. PMID: 20305726 Free PMC article.
-
Comparison of optical coherence tomography and ultrasound biomicroscopy for detection of narrow anterior chamber angles.Arch Ophthalmol. 2005 Aug;123(8):1053-9. doi: 10.1001/archopht.123.8.1053. Arch Ophthalmol. 2005. PMID: 16087837
-
Comparison of ultrasound biomicroscopy and spectral-domain anterior segment optical coherence tomography in evaluation of anterior segment after laser peripheral iridotomy.Int J Ophthalmol. 2016 Mar 18;9(3):417-23. doi: 10.18240/ijo.2016.03.16. eCollection 2016. Int J Ophthalmol. 2016. PMID: 27158613 Free PMC article.
-
Angle imaging: advances and challenges.Indian J Ophthalmol. 2011 Jan;59 Suppl(Suppl1):S69-75. doi: 10.4103/0301-4738.73699. Indian J Ophthalmol. 2011. PMID: 21150037 Free PMC article. Review.
-
Evaluation of the anterior chamber angle in glaucoma: a report by the american academy of ophthalmology.Ophthalmology. 2013 Oct;120(10):1985-97. doi: 10.1016/j.ophtha.2013.05.034. Epub 2013 Aug 23. Ophthalmology. 2013. PMID: 23978623 Review.
Cited by
-
Detection of primary angleclosure suspect with different mechanisms of angle closure using multivariate prediction models.Acta Ophthalmol. 2021 Jun;99(4):e576-e586. doi: 10.1111/aos.14634. Epub 2020 Sep 30. Acta Ophthalmol. 2021. PMID: 32996707 Free PMC article.
-
Ultrasound biomicroscopy in glaucoma assessment.Rom J Ophthalmol. 2021 Apr-Jun;65(2):114-119. doi: 10.22336/rjo.2021.24. Rom J Ophthalmol. 2021. PMID: 34179574 Free PMC article. Review.
-
Deep Learning for Anterior Segment Optical Coherence Tomography to Predict the Presence of Plateau Iris.Transl Vis Sci Technol. 2021 Jan 6;10(1):7. doi: 10.1167/tvst.10.1.7. eCollection 2021 Jan. Transl Vis Sci Technol. 2021. PMID: 33505774 Free PMC article.
-
Diagnostic performance of anterior segment optical coherence tomography in detecting plateau iris.BMJ Open Ophthalmol. 2022 Mar 23;7(1):e000931. doi: 10.1136/bmjophth-2021-000931. eCollection 2022. BMJ Open Ophthalmol. 2022. PMID: 35402728 Free PMC article.
-
Can ultrasonic biometric indices with optimal cut-offs be a potential screening tool for primary angle closure disease? A case-control study.Eye (Lond). 2023 Apr;37(6):1284-1289. doi: 10.1038/s41433-022-02118-y. Epub 2022 May 27. Eye (Lond). 2023. PMID: 35624303 Free PMC article.
References
-
- American Academy of Ophthalmology. Primary Angle Closure, Preferred Practice Pattern. San Francisco, Calif, USA: American Academy of Ophthalmology; 2005.
-
- Dandona L, Dandona R, Mandal P, et al. Angle-closure glaucoma in an urban population in Southern India: the andhra pradesh eye disease study. Ophthalmology. 2000;107(9):1710–1716. - PubMed
-
- Jacob A, Thomas R, Koshi SP, Braganza A, Muliyil J. Prevalence of primary glaucoma in an urban South Indian population. Indian Journal of Ophthalmology. 1998;46(2):81–86. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials