

The association between "hypertriglyceridemic waist" and sub-clinical atherosclerosis in a multiethnic population: a cross-sectional study
- PMID: 24558974
- PMCID: PMC3938067
- DOI: 10.1186/1476-511X-13-38
The association between "hypertriglyceridemic waist" and sub-clinical atherosclerosis in a multiethnic population: a cross-sectional study
Abstract
Background: "Hypertriglyceridemic waist" (HTGW) phenotype, an inexpensive early screening tool for detection of individuals at risk for type 2 diabetes and cardiovascular disease was found to be associated with subclinical atherosclerosis in various patient populations such as those with diabetes mellitus, chronic kidney disease, and those infected with human immunodeficiency virus. However, less is known regarding an association between HTGW and subclinical atherosclerosis in the apparently healthy, multiethnic population. Therefore, the aim of the study was to explore the association between HTGW and sub-clinical atherosclerosis in an apparently healthy, multiethnic population; and to investigate whether the effect of HTGW on sub-clinical atherosclerosis persists over and above the traditional atherosclerosis risk factors.
Methods: We studied 809 individuals of Aboriginal, Chinese, European and South Asian origin who were assessed for indices of sub-clinical atherosclerosis (intima-media thickness (IMT), total area and presence of carotid plaques), socio-demographic and lifestyle characteristics, anthropometrics, lipids, glucose, blood pressure, and family history of cardiovascular disease.
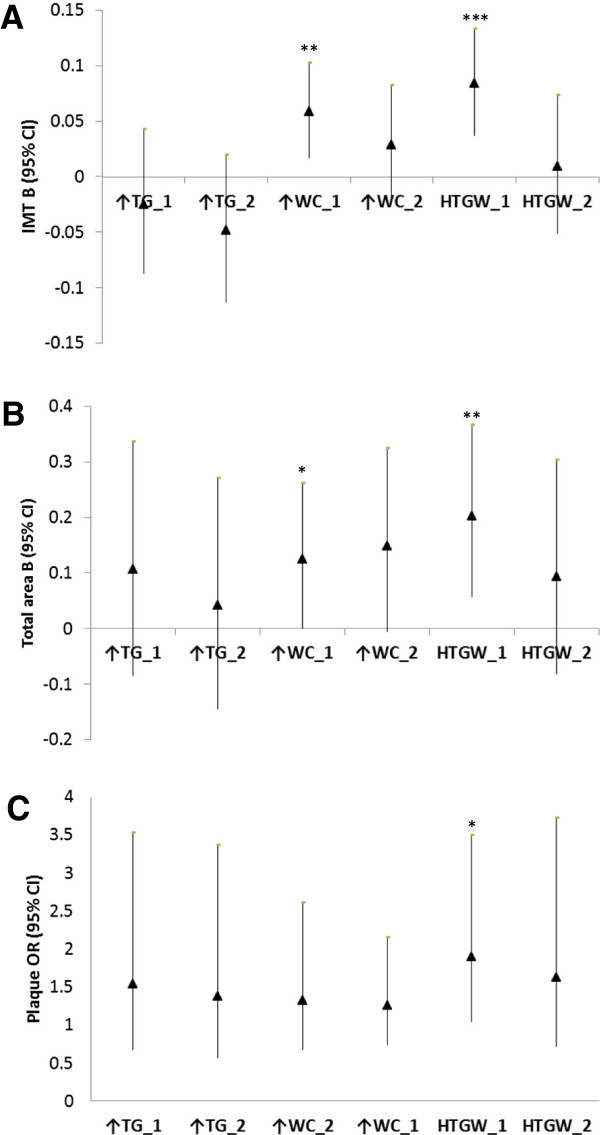
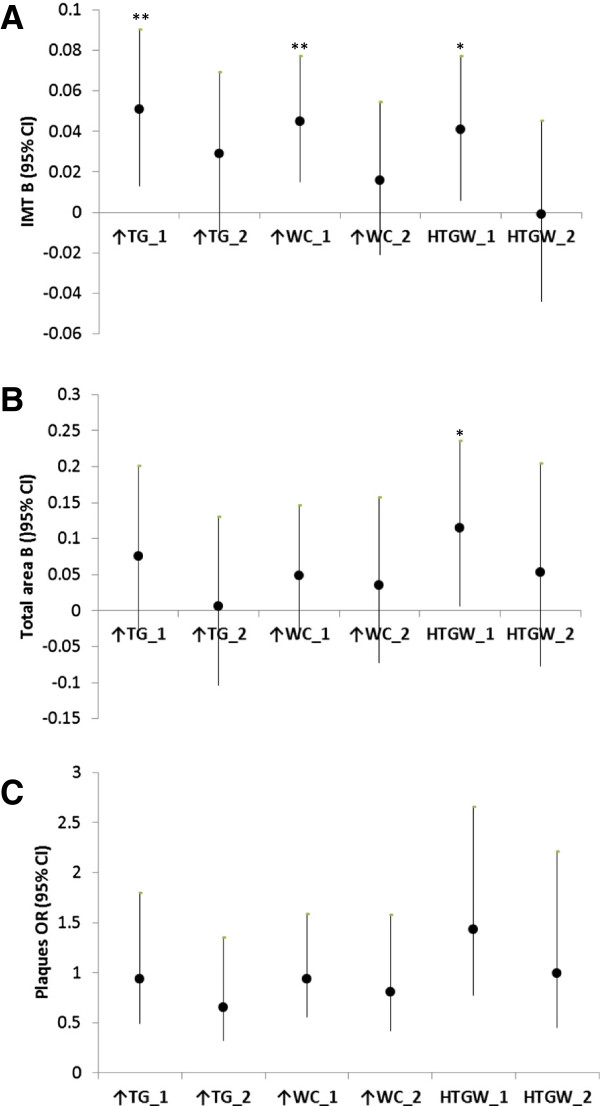
Results: We found that, compared to individuals without HTGW and after adjusting for age, ethnicity, smoking, and physical activity; men and women with HTGW had a significantly higher: IMT (men: B (95%CI = 0.084 (0.037, 1.133), p < 0.001; women: B (95%CI) = 0.041 (0.006, 0.077), p = 0.020); and total area (men: B (95%CI = 0.202 (0.058, 0.366), p = 0.005; women: B (95%CI) = 0.115 (0.006, 0.235), p = 0.037). The association between HTGW waist and presence of plaques was significant for men (OR (95%CI) = 1.904 (1.040, 3.486), p = 0.037 vs. men without HTGW), but not for women (p = 0.284). Once analyses were adjusted for additional, traditional risk factors for atherosclerosis, the effect of HTGW on sub-clinical atherosclerosis was no longer significant.
Conclusions: In conclusion, HTGW may serve as an early marker of subclinical atherosclerosis in men and women, irrespective of ethnicity. However, once individuals are assessed for all traditional risk factors for atherosclerosis, the additional assessment for HTGW is not warranted.
Figures
References
-
- O’Leary DH, Polak JF, Kronmal RA, Manolio TA, Burke GL, Wolfson SK Jr. Carotid-artery intima and media thickness as a risk factor for myocardial infarction and stroke in older adults. Cardiovasc Health Study Collaborative Res Group NEJM. 1999;340:14–22. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
