

Podocin and beta dystroglycan expression to study podocyte-podocyte and basement membrane matrix connections in adult protienuric states
- PMID: 24559085
- PMCID: PMC3996081
- DOI: 10.1186/1746-1596-9-40
Podocin and beta dystroglycan expression to study podocyte-podocyte and basement membrane matrix connections in adult protienuric states
Abstract
Background: Podocytes can be the primary site of injury or secondarily involved in various protienuric states. Cross talk between adjacent foot processes and with basement membrane is important for slit diaphragm function. Does expression of podocyte associated proteins in kidney biopsies alter with site/type of primary injury? Genetic mutations of podocin result in steroid resistant FSGS. Can protein expression of podocin predict resistant cases to initiate further genetic evaluation?
Methods: Adult patients (n-88) with protienuria- minimal change disease(MCD)-22, focal segmental glomerulosclerosis(FSGS)-21,membranous glomerulonephritis(MGN)-25 and IgA nephropathy(IgAN)-20 were selected for immunohistochemistry with podocin and beta dystroglycan . Results were graded (0 - 3+scale )and compared with control biopsies and internal control. Treatment and follow up (6 months -2 ½ years) of FSGS and MCD cases were collected.
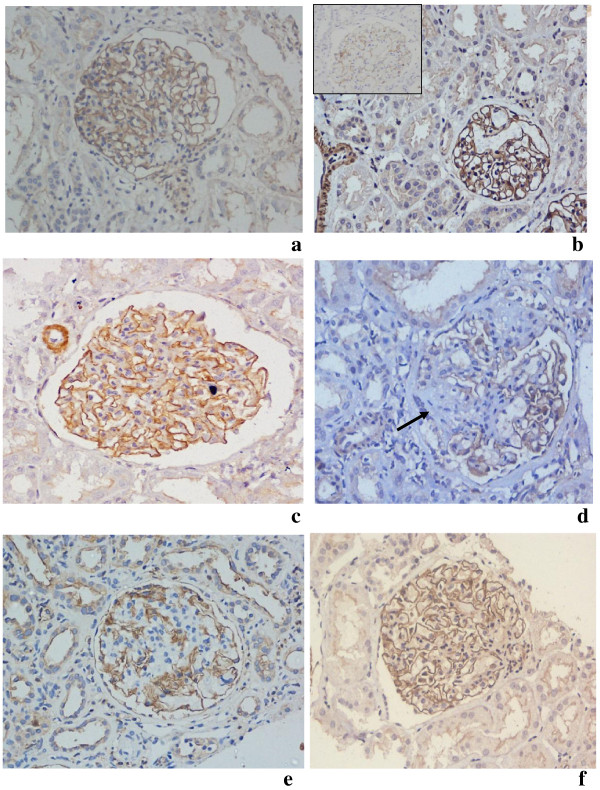
Results: There was intense to moderate staining of the podocytes with podocin and β dystroglycan in the glomeruli in all cases (MCD, FSGS, IgAN and MGN) except for weak staining with β dystroglycan in 3 cases of MCD. There was loss of immunostains in areas of segmental/global sclerosis. There was no significant difference in the staining pattern between the groups. In primary podocytopathies, staining pattern did not differ between steroid resistant, sensitive or dependent cases.
Conclusions: Immunohistochemical expression of podocin and β dystroglycan does not differ in nephropathies which have different site of injury depending on absence (MCD and FSGS) or presence of immune deposits and their localization (MGN and IgAN). Podocin and β dystroglycan staining did not differentiate steroid sensitive and resistant cases, hence, does not give clue to initiate genetic studies. However, analysis of bigger cohort may be required.
Summary: Podocin and β dystroglycan immunohistochemistry was done to analyze podocyte - podocyte and podocyte -basement membrane matrix connections in adult protienuric states. Primary podocytopathies i.e. MCD and FSGS and secondary podocytopathy due to immune complex deposition, i.e., MGN (subepithelial) and IgAN (mesangial) were analyzed. There was no difference in staining patterns between primary and secondary podocytopathies or between steroid sensitive, resistant and dependent cases of FSGS and MCD.
Virtual slides: The virtual slide(s) for this article can be found here: http://www.diagnosticpathology.diagnomx.eu/vs/2258608781052786.
Figures

Similar articles
-
Reduced podocin expression in minimal change disease and focal segmental glomerulosclerosis is related to the level of proteinuria.Clin Exp Nephrol. 2013 Dec;17(6):811-8. doi: 10.1007/s10157-013-0775-y. Epub 2013 Feb 2. Clin Exp Nephrol. 2013. PMID: 23377573
-
Dystroglycan in the diagnosis of FSGS.Clin J Am Soc Nephrol. 2009 Nov;4(11):1747-53. doi: 10.2215/CJN.01510209. Epub 2009 Sep 24. Clin J Am Soc Nephrol. 2009. PMID: 19808230 Free PMC article.
-
Gene expression profiles of podocyte-associated molecules as diagnostic markers in acquired proteinuric diseases.J Am Soc Nephrol. 2003 Nov;14(11):2958-66. doi: 10.1097/01.asn.0000090745.85482.06. J Am Soc Nephrol. 2003. PMID: 14569107
-
Approach to Diagnosis and Management of Primary Glomerular Diseases Due to Podocytopathies in Adults: Core Curriculum 2020.Am J Kidney Dis. 2020 Jun;75(6):955-964. doi: 10.1053/j.ajkd.2019.12.019. Epub 2020 Apr 21. Am J Kidney Dis. 2020. PMID: 32331832 Review.
-
Targeting podocyte-associated diseases.Adv Drug Deliv Rev. 2010 Nov 30;62(14):1325-36. doi: 10.1016/j.addr.2010.08.012. Epub 2010 Sep 7. Adv Drug Deliv Rev. 2010. PMID: 20828590 Review.
Cited by
-
Biomarkers in Primary Focal Segmental Glomerulosclerosis in Optimal Diagnostic-Therapeutic Strategy.J Clin Med. 2022 Jun 8;11(12):3292. doi: 10.3390/jcm11123292. J Clin Med. 2022. PMID: 35743361 Free PMC article. Review.
References
-
- Regele Hm FE, Langer B, Poczewki H, Kraxberger I, Bittner Re, Kerjaschki D. Glomerular Expression of Dystroglycans Is Reduced in Minimal Change Nephrosis But Not in Focal Segmental Glomerulosclerosis. J Am Soc Nephrol. 2000;11:403–412. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
