

Pressure ulcer multidisciplinary teams via telemedicine: a pragmatic cluster randomized stepped wedge trial in long term care
- PMID: 24559218
- PMCID: PMC4104322
- DOI: 10.1186/1472-6963-14-83
Pressure ulcer multidisciplinary teams via telemedicine: a pragmatic cluster randomized stepped wedge trial in long term care
Abstract
Background: The study was conducted to determine the clinical and cost effectiveness of enhanced multi-disciplinary teams (EMDTs) vs. 'usual care' for the treatment of pressure ulcers in long term care (LTC) facilities in Ontario, Canada
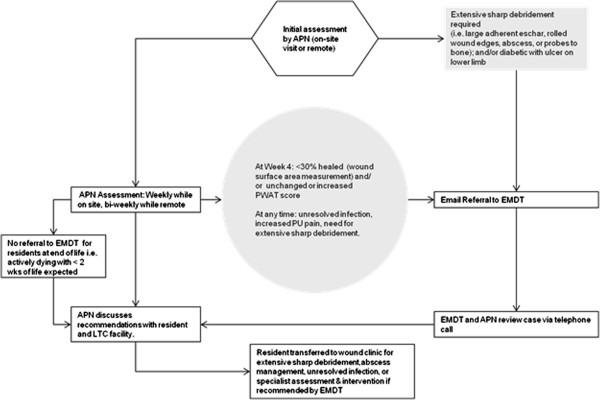
Methods: We conducted a multi-method study: a pragmatic cluster randomized stepped-wedge trial, ethnographic observation and in-depth interviews, and an economic evaluation. Long term care facilities (clusters) were randomly allocated to start dates of the intervention. An advance practice nurse (APN) with expertise in skin and wound care visited intervention facilities to educate staff on pressure ulcer prevention and treatment, supported by an off-site hospital based expert multi-disciplinary wound care team via email, telephone, or video link as needed. The primary outcome was rate of reduction in pressure ulcer surface area (cm2/day) measured on before and after standard photographs by an assessor blinded to facility allocation. Secondary outcomes were time to healing, probability of healing, pressure ulcer incidence, pressure ulcer prevalence, wound pain, hospitalization, emergency department visits, utility, and cost.
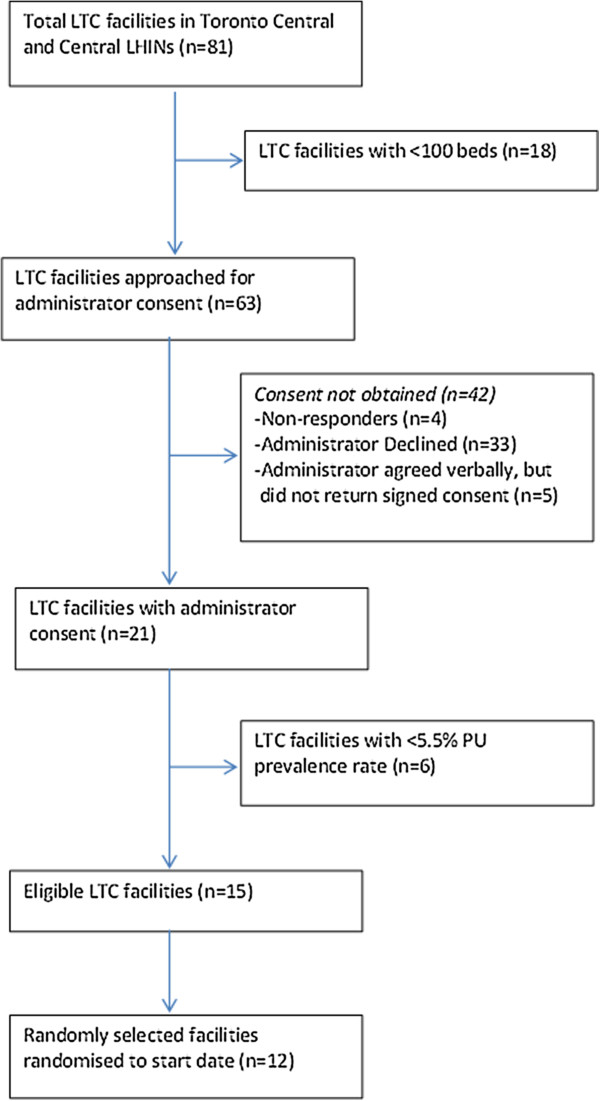
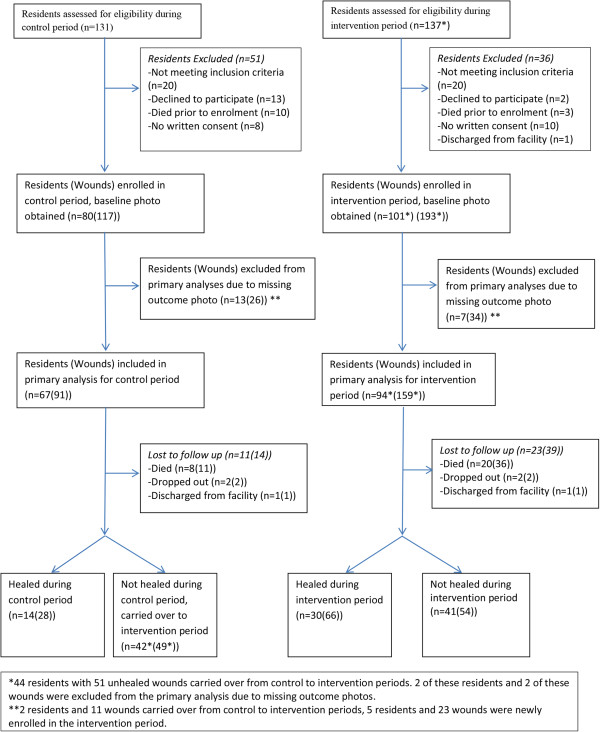
Results: 12 of 15 eligible LTC facilities were randomly selected to participate and randomized to start date of the intervention following the stepped wedge design. 137 residents with a total of 259 pressure ulcers (stage 2 or greater) were recruited over the 17 month study period. No statistically significant differences were found between control and intervention periods on any of the primary or secondary outcomes. The economic evaluation demonstrated a mean reduction in direct care costs of $650 per resident compared to 'usual care'. The qualitative study suggested that onsite support by APN wound specialists was welcomed, and is responsible for reduced costs through discontinuation of expensive non evidence based treatments. Insufficient allocation of nursing home staff time to wound care may explain the lack of impact on healing.
Conclusion: Enhanced multi-disciplinary wound care teams were cost effective, with most benefit through cost reduction initiated by APNs, but did not improve the treatment of pressure ulcers in nursing homes. Policy makers should consider the potential yield of strengthening evidence based primary care within LTC facilities, through outreach by APNs.
Trial registration: ClinicalTrials.gov identifier NCT01232764.
Figures
References
-
- National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel. Prevention and treatment of pressure ulcers: clinical practice guideline. Washington (DC): National Pressure Ulcer Advisory Panel; 2009. Pressure ulcer treatment recommendations; pp. 51–120.
-
- Horn SD, Bender SA, Ferguson ML, Smout RJ, Bergstrom N, Taler G, Cook AS, Sharkey SS, Coble Voss A. The national pressure ulcer long-term care study: pressure ulcer development in long-term care residents. J Am Geriatr Soc. 2004;14:359–367. - PubMed
-
- Woodbury MG, Houghton PE. Prevalence of Pressure Ulcers in Canadian Health Care Settings. Ostomy Wound Management. 2004;14(10):22–38. - PubMed
-
- Cuddigan J, Berlowitz DR, Ayello EA. Pressure ulcers in America: Prevalence, incidence and implications for future: an executive summary of the National Pressure Ulcer Advisory Panel Monograph. Adv Skin Wound Care. 2001;14:208–215. - PubMed
-
- Bennett G, Dealey C, Posnett J. The cost of pressure ulcers in the UK. Age Ageing. 2004;14(3):230–235. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
