

The clinical implications of the oblique retinacular ligament
- PMID: 24559632
- PMCID: PMC3977782
- DOI: 10.1016/j.jhsa.2013.12.011
The clinical implications of the oblique retinacular ligament
Abstract
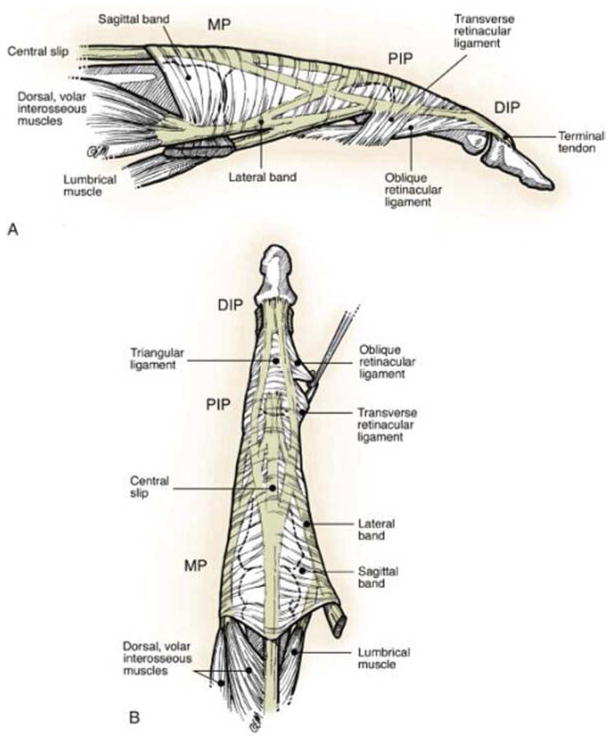
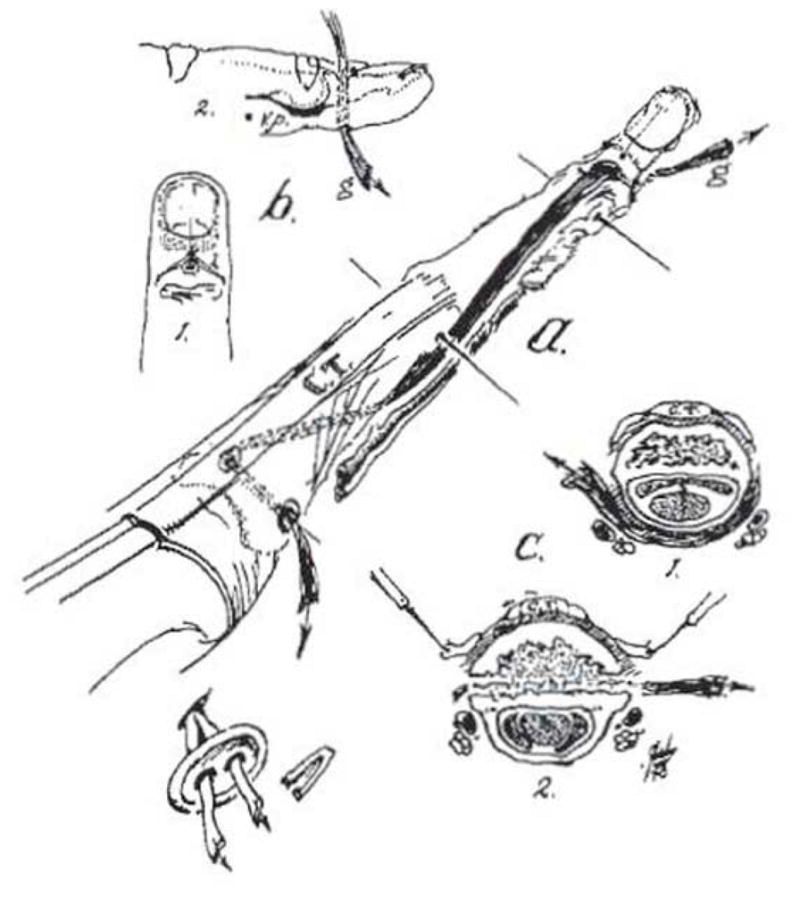
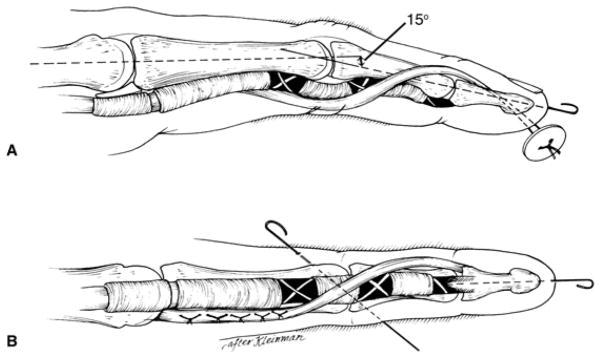
The oblique retinacular ligament originates from the flexor tendon sheath, courses past the proximal interphalangeal joint, and merges with the lateral extensor tendon. There has been disagreement regarding the contribution of the oblique retinacular ligament to coordinated movements between the proximal and distal interphalangeal joints. Landsmeer postulated that it acts as a dynamic tenodesis that tightens with proximal interphalangeal joint extension, causing obligatory distal interphalangeal joint extension. However, studies have shown that the oblique retinacular ligament is variably present and often attenuated, which diminishes its presumed role in finger movement. Despite this, the concept of a checkrein linking interphalangeal joint motion heralded the development of effective and reproducible surgical interventions for swan-neck and mallet deformities. This article examines the controversy regarding the existence of the oblique retinacular ligament, its plausible functionality, and clinical implications in the practice of hand surgery.
Keywords: Oblique retinacular ligament; mallet finger; swan-neck.
Copyright © 2014 American Society for Surgery of the Hand. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Spiral Oblique Retinacular Ligament Procedure Using Flexor Digitorum Profundus Hemi-Tendon Transfer: Anatomical Basis and Clinical Application.J Hand Surg Am. 2021 Nov;46(11):1023.e1-1023.e7. doi: 10.1016/j.jhsa.2021.02.018. Epub 2021 Apr 15. J Hand Surg Am. 2021. PMID: 33865656
-
Acute Traumatic Swan Neck Deformity: A Case Report of the Oblique Retinacular Ligament Lesion.J Hand Surg Asian Pac Vol. 2017 Sep;22(3):359-362. doi: 10.1142/S0218810417720236. J Hand Surg Asian Pac Vol. 2017. PMID: 28774252
-
Anatomy of the oblique retinacular ligament of the index finger.J Hand Surg Am. 1993 Jul;18(4):717-21. doi: 10.1016/0363-5023(93)90326-X. J Hand Surg Am. 1993. PMID: 8349989
-
Managing Swan Neck and Boutonniere Deformities.Clin Plast Surg. 2019 Jul;46(3):329-337. doi: 10.1016/j.cps.2019.02.006. Epub 2019 Apr 16. Clin Plast Surg. 2019. PMID: 31103077 Review.
-
Surgical treatment of chronic mallet finger.Ann Plast Surg. 2011 Jun;66(6):670-2. doi: 10.1097/SAP.0b013e3181e6d017. Ann Plast Surg. 2011. PMID: 21467915 Review.
Cited by
-
[Ligamentous lesions and instability of the finger joints].Orthopade. 2018 Feb;47(2):175-188. doi: 10.1007/s00132-017-3510-7. Orthopade. 2018. PMID: 29264616 Review. German.
-
Anatomy of Landsmeer Ligaments-Redefined.Indian J Plast Surg. 2019 May;52(2):195-200. doi: 10.1055/s-0039-1695802. Epub 2019 Sep 10. Indian J Plast Surg. 2019. PMID: 31602135 Free PMC article.
-
Spiral oblique retinacular ligament reconstruction using lateral band technique to treat swan neck deformity due to chronic mallet finger: A case report.Int J Surg Case Rep. 2021 Apr;81:105811. doi: 10.1016/j.ijscr.2021.105811. Epub 2021 Mar 26. Int J Surg Case Rep. 2021. PMID: 33887839 Free PMC article.
References
-
- Littler JW. The finger extensor mechanism. Surg Clin North Am. 1967;47:415–432. - PubMed
-
- Kaplan EB. Functional and surgical anatomy of the hand. 2. Philadelphia, PA: J.B. Lippincott Co; 1965. pp. 42–43.
-
- Harris C, Jr, Rutledge GL., Jr The functional anatomy of the extensor mechanism of the finger. J Bone Joint Surg. 1972;54A:713–726. - PubMed
-
- Ulrich F, Schmidt HM. Deep Ligaments of the interphalangeal joint of the thumb. Nato Adv Sci Inst Se. 1994;256:69–84.
-
- Weitbrecht J. Syndesmology; or, A description of the ligaments of the human body, arranged in accordance with anatomical dissections and illustrated with figures drawn from fresh subjects. University of Otago; NZ: 1742. Retrieved August 2013.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
