

Ethanol infusion in the vein of Marshall leads to parasympathetic denervation of the human left atrium: implications for atrial fibrillation
- PMID: 24561151
- PMCID: PMC4035125
- DOI: 10.1016/j.jacc.2014.01.032
Ethanol infusion in the vein of Marshall leads to parasympathetic denervation of the human left atrium: implications for atrial fibrillation
Abstract
Objectives: This study sought to determine whether ethanol infusion in the vein of Marshall (VOM) can ablate intrinsic cardiac nerves (ICN).
Background: ICN cluster around the left atrial epicardium and are implicated in the genesis of atrial fibrillation (AF).
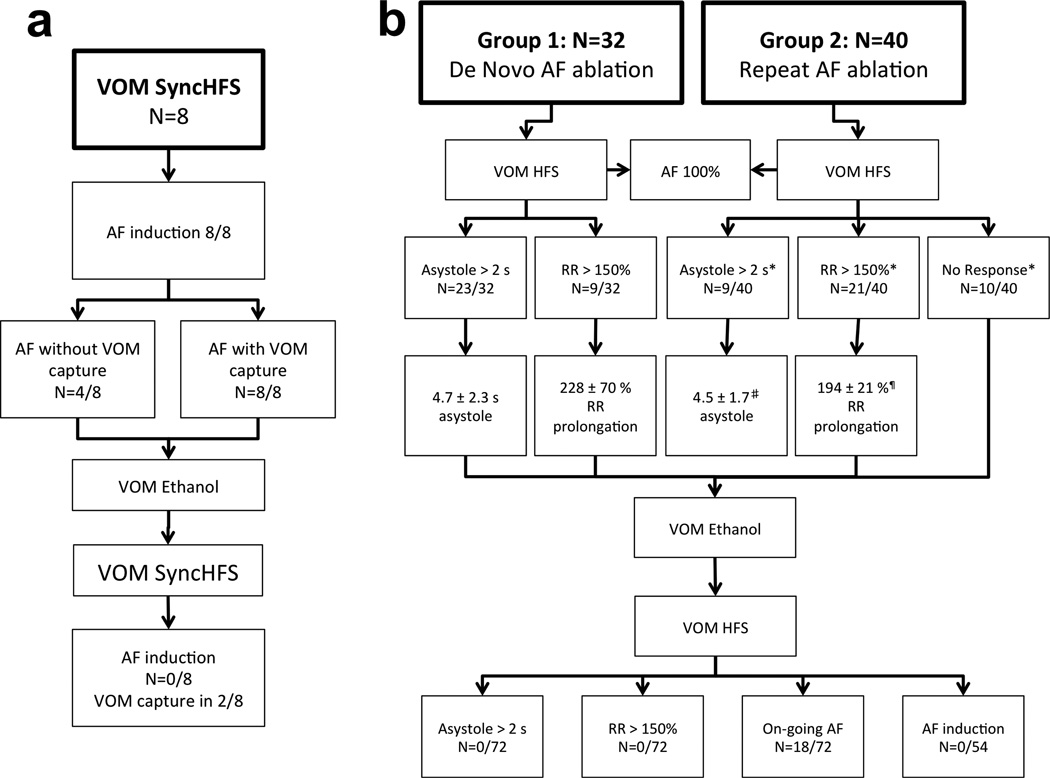
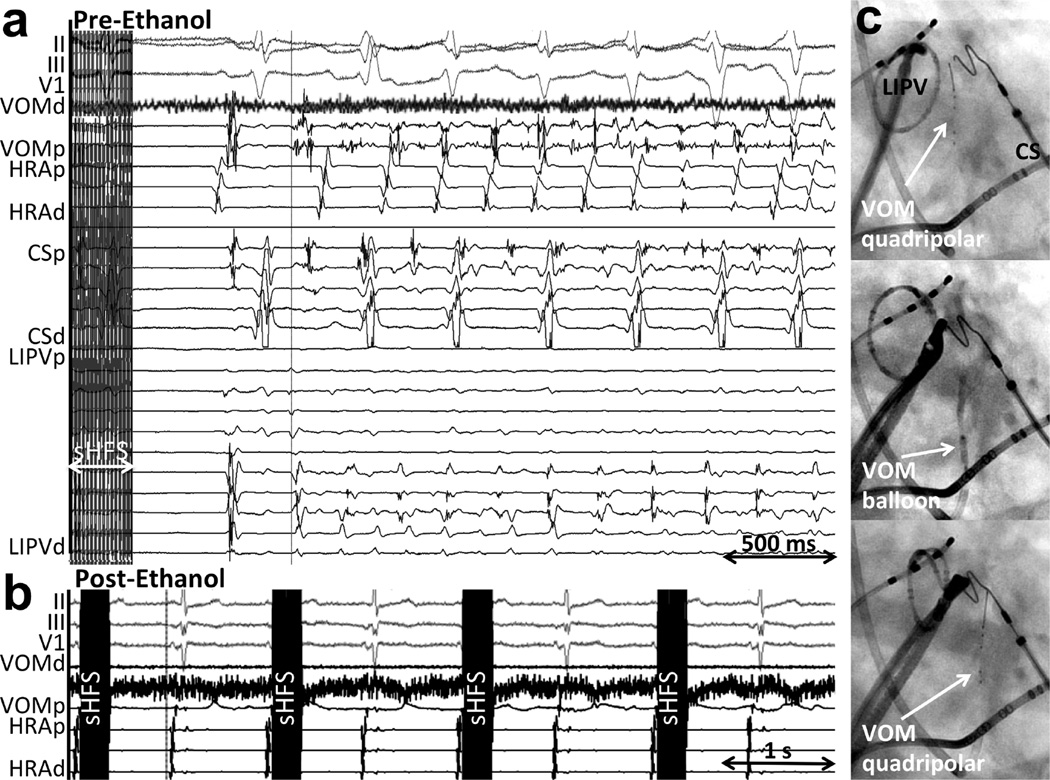
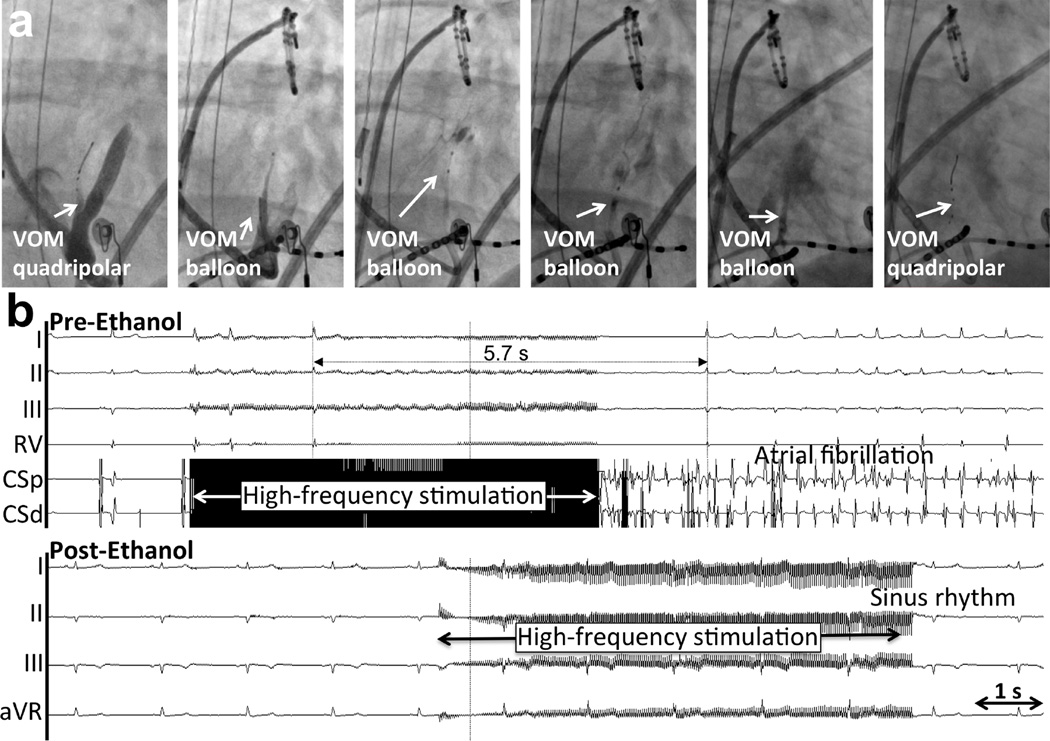
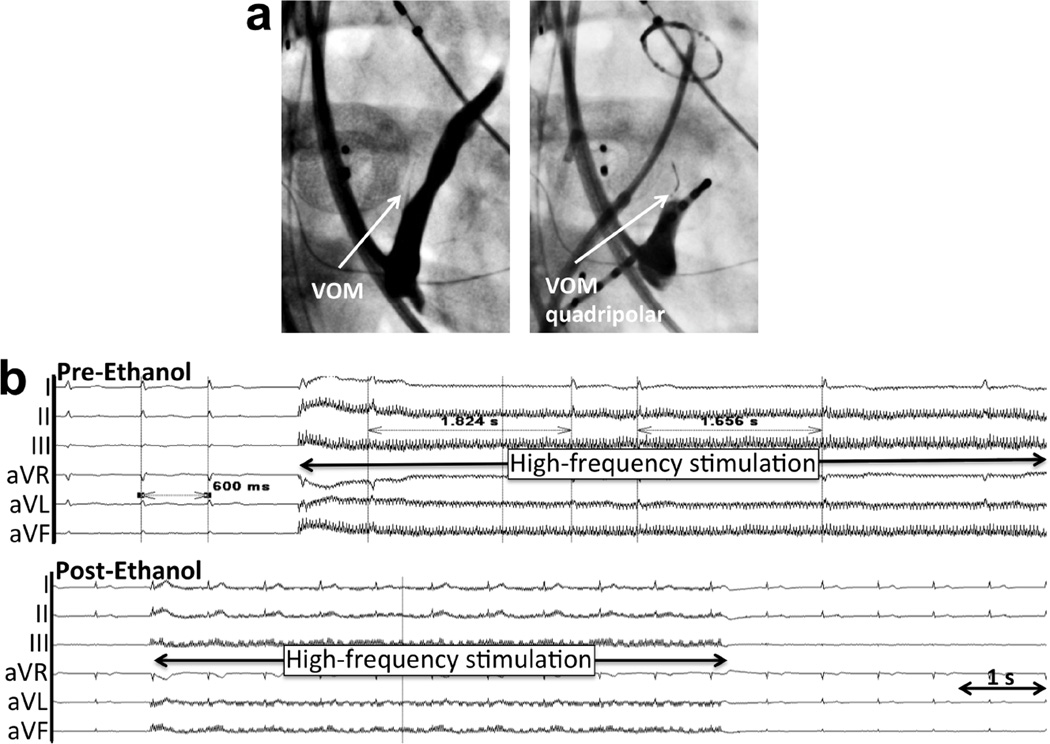
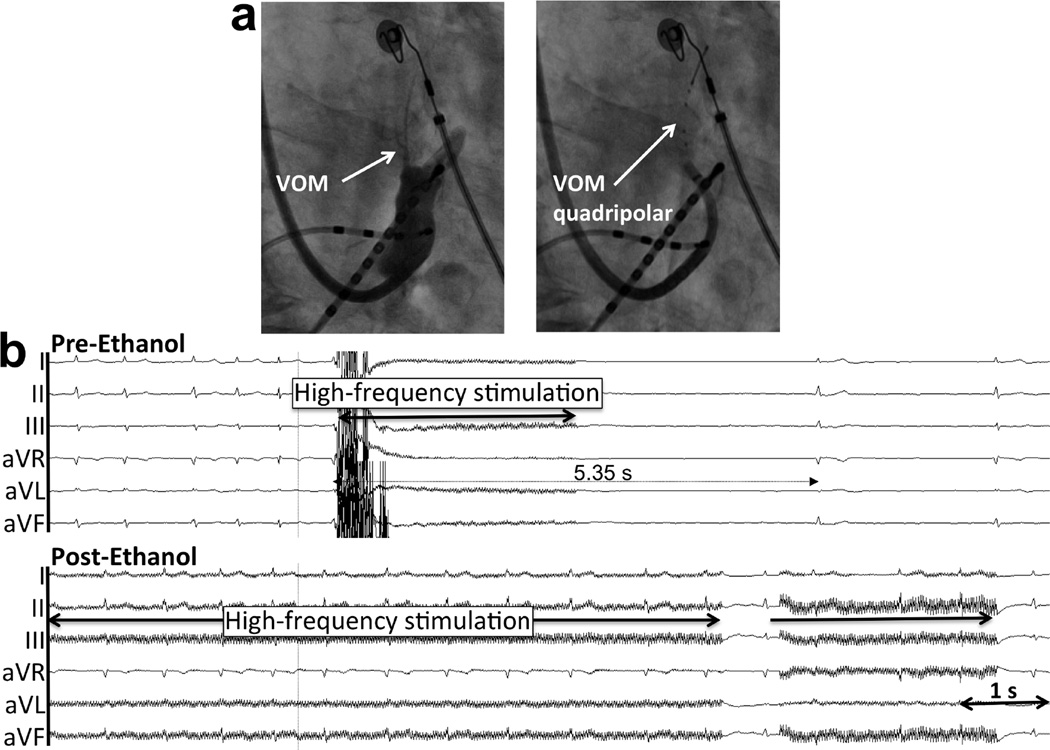
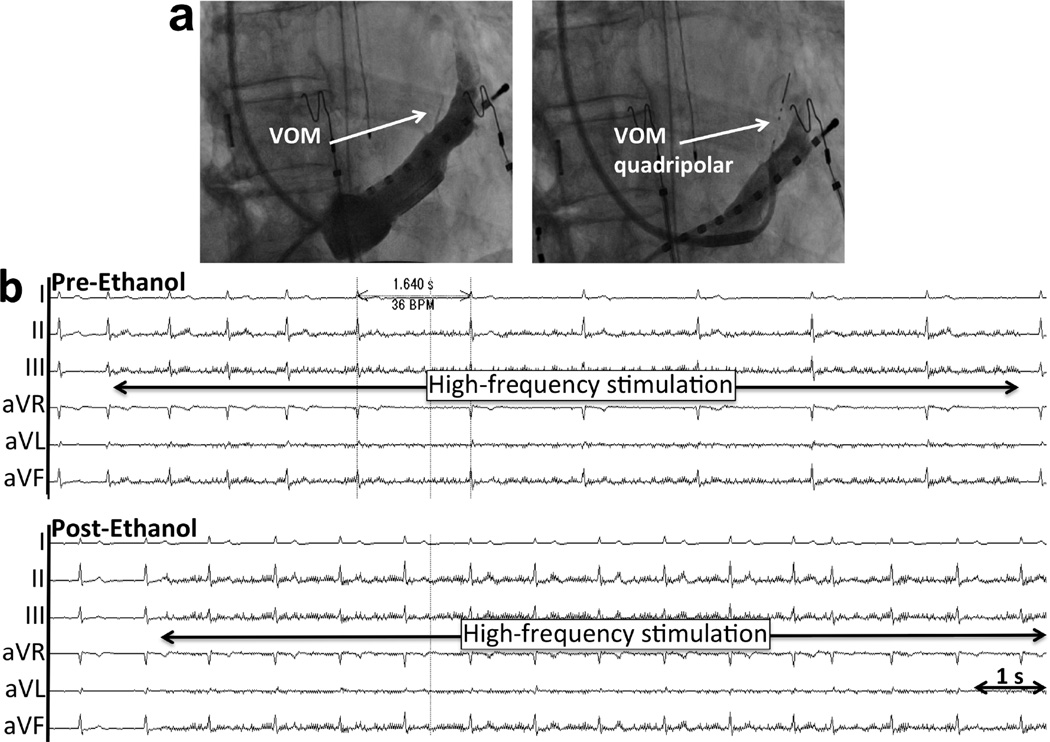
Methods: Patients undergoing catheter AF ablation underwent adjunctive ethanol injection in the VOM. A multipolar catheter was introduced in the VOM and used for high-frequency stimulation (HFS), either as HFS with P-wave synchronized (SynchHFS), 30 pulses, 100 Hz (n = 8) or as HFS with 3 to 10 s bursts (BurstHFS), 33 Hz (n = 72) at 25 mA for 1-ms duration. Atrioventricular (AV) nodal conduction slowing (asystole >2 s or R-R interval prolongation >50%) and AF inducibility were assessed before and after VOM ethanol infusion. Up to 4 1-ml infusions of 98% ethanol were delivered via an angioplasty balloon in the VOM.
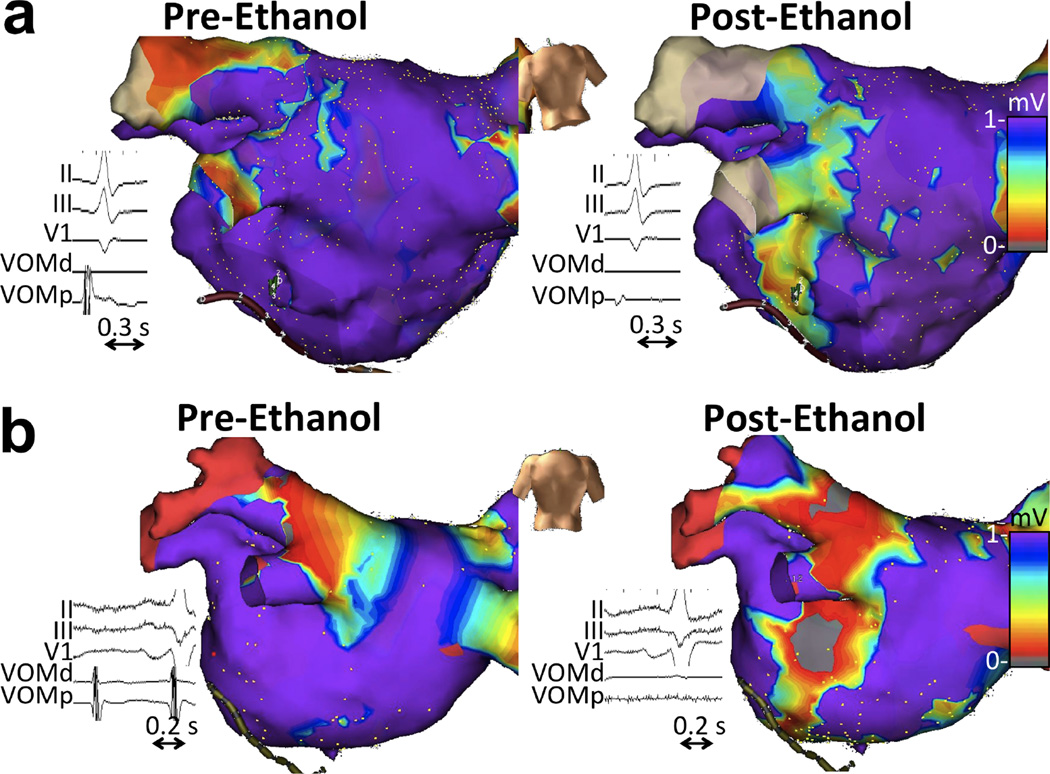
Results: SynchHFS induced AF in 8 of 8 patients. In 4 of 8 AF initiated spontaneously without VOM capture. No parasympathetic responses were elicited by SynchHFS. BurstHFS was performed in 32 patients undergoing de novo AF ablation (Group 1) and 40 patients undergoing repeat ablation (Group 2). Parasympathetic responses were found in all 32 Group 1 patients and in 75% of Group 2 patients. After VOM ethanol infusion, parasympathetic responses were abolished in all patients (both groups). There were no acute complications related to VOM ethanol infusion.
Conclusions: The VOM contains ICN that connect with the AV node and can trigger AF. Retrograde ethanol infusion in the VOM reliably eliminates local ICN responses. The VOM is a vascular route for ICN-targeting therapies.
Keywords: atrial fibrillation; ethanol; intrinsic cardiac nerves; vein of Marshall.
Copyright © 2014 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Marshaling the autonomic nervous system for treatment of atrial fibrillation.J Am Coll Cardiol. 2014 May 13;63(18):1902-3. doi: 10.1016/j.jacc.2014.01.033. Epub 2014 Feb 19. J Am Coll Cardiol. 2014. PMID: 24561143 Free PMC article. No abstract available.
References
-
- Katritsis DG, Giazitzoglou E, Zografos T, Pokushalov E, Po SS, Camm AJ. Rapid pulmonary vein isolation combined with autonomic ganglia modification: a randomized study. Heart Rhythm. 2011;8:672–678. - PubMed
-
- Nakagawa H, Scherlag BJ, Patterson E, Ikeda A, Lockwood D, Jackman WM. Pathophysiologic basis of autonomic ganglionated plexus ablation in patients with atrial fibrillation. Heart Rhythm. 2009;6:S26–S34. - PubMed
-
- Calkins H, Kuck KH, Cappato R, et al. 2012 HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design: a report of the Heart Rhythm Society (HRS) Task Force on Catheter and Surgical Ablation of Atrial Fibrillation. Heart Rhythm. 2012;9:632–696. e21. - PubMed
-
- Kim DT, Lai AC, Hwang C, et al. The ligament of Marshall: a structural analysis in human hearts with implications for atrial arrhythmias. Journal of the American College of Cardiology. 2000;36:1324–1327. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
