

Diagnostic accuracy of combined cardiac troponin and copeptin assessment for early rule-out of myocardial infarction: a systematic review and meta-analysis
- PMID: 24562800
- PMCID: PMC3932778
- DOI: 10.1177/2048872613514015
Diagnostic accuracy of combined cardiac troponin and copeptin assessment for early rule-out of myocardial infarction: a systematic review and meta-analysis
Abstract
Aims: This systematic review aimed to investigate the diagnostic accuracy of combined cardiac troponin (cTn) and copeptin assessment in comparison to cTn alone for early rule-out of acute myocardial infarction (AMI).
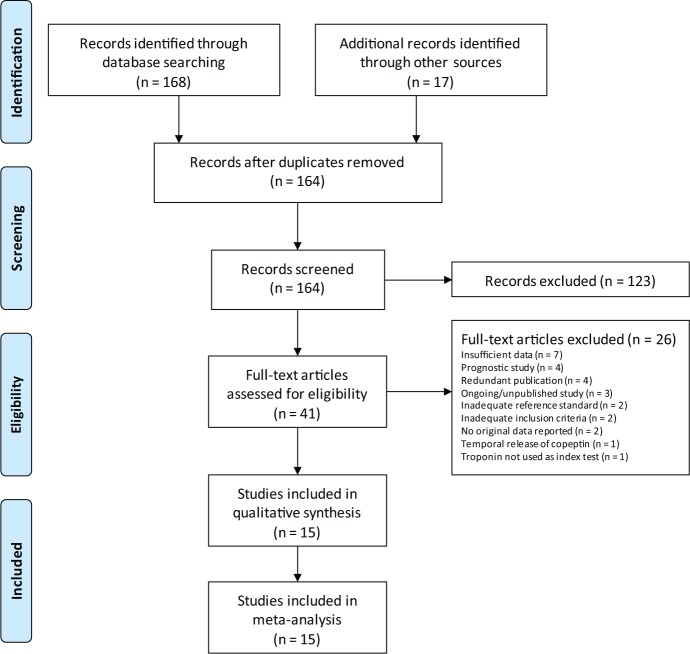
Methods: Primary studies were eligible if they evaluated diagnostic accuracy for cTn with and without copeptin in patients with symptoms suggestive of AMI. AMI was defined according to the universal definition, using detection of cTn as a marker for myocardial necrosis. Eligible studies were identified by searching electronic databases (Medline, EMBASE, Science Citation Index Expanded, CINAHL, Pascal, and Cochrane) from inception to March 2013, reviewing conference proceedings and contacting field experts and the copeptin manufacturer.
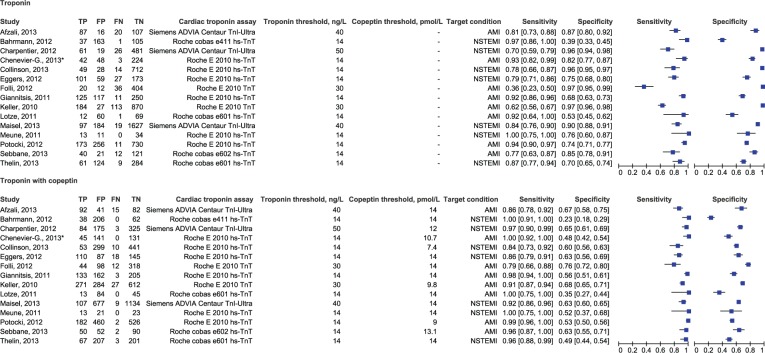
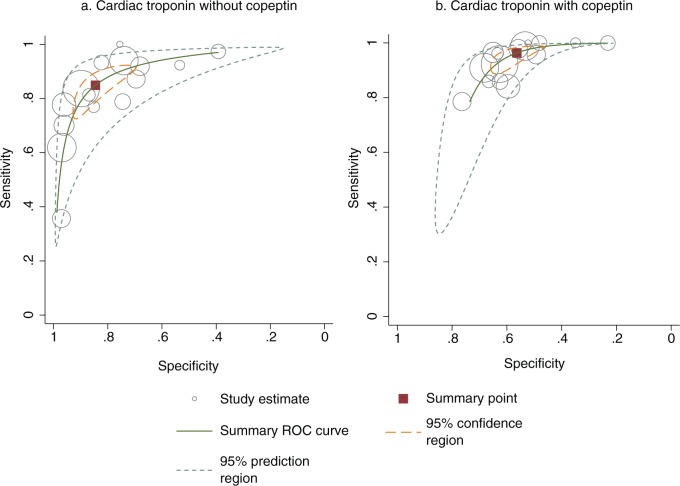
Results: In 15 studies totalling 8740 patients (prevalence of AMI 16%), adding copeptin improved the sensitivity of cTn assays (from 0.87 to 0.96, p=0.003) at the expense of lower specificity (from 0.84 to 0.56, p<0.001). In 12 studies providing data for 6988 patients without ST-segment elevation, the summary sensitivity and specificity estimates were 0.95 (95% CI 0.89 to 0.98) and 0.57 (95% CI 0.49 to 0.65) for the combined assessment of cTn and copeptin. When a high-sensitivity cTnT assay was used in combination with copeptin, the summary sensitivity and specificity estimates were 0.98 (95% CI 0.96 to 1.00) and 0.50 (95% CI 0.42 to 0.58).
Conclusion: Despite substantial between-study heterogeneity, this meta-analysis demonstrates that copeptin significantly improves baseline cTn sensitivity. Management studies are needed to establish the effectiveness and safety of measuring copeptin in combination with high-sensitivity cTnT for early rule-out of AMI without serial testing.
Keywords: copeptin; diagnostic accuracy; myocardial infarction; troponin.
Conflict of interest statement
Figures
References
-
- Hamm CW, Bassand JP, Agewall S, et al. ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: the Task Force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J 2011; 32: 2999–3054 - PubMed
-
- Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of myocardial infarction. Eur Heart J 2012; 33: 2551–2567 - PubMed
-
- Reichlin T, Hochholzer W, Stelzig C, et al. Incremental value of copeptin for rapid rule out of acute myocardial infarction. J Am Coll Cardiol 2009; 54: 60–68 - PubMed
-
- Morgenthaler NG, Struck J, Alonso C, et al. Assay for the measurement of copeptin, a stable peptide derived from the precursor of vasopressin. Clin Chem 2006; 52: 112–119 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
