

Transient attenuation of the amplitude of the QRS complexes in the diagnosis of Takotsubo syndrome
- PMID: 24562801
- PMCID: PMC3932773
- DOI: 10.1177/2048872613504311
Transient attenuation of the amplitude of the QRS complexes in the diagnosis of Takotsubo syndrome
Abstract
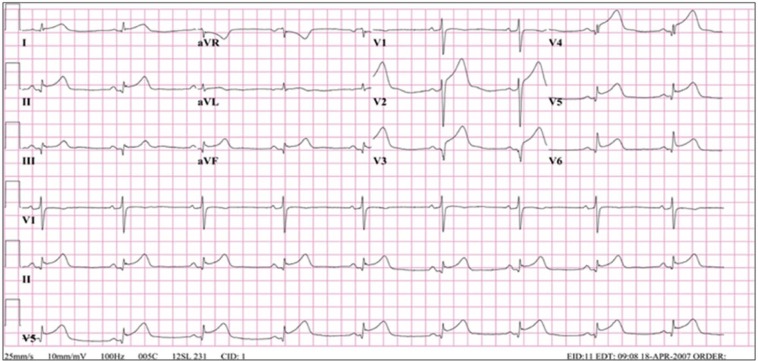
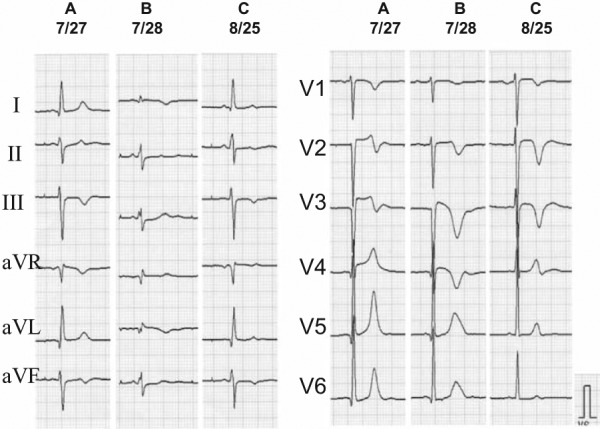
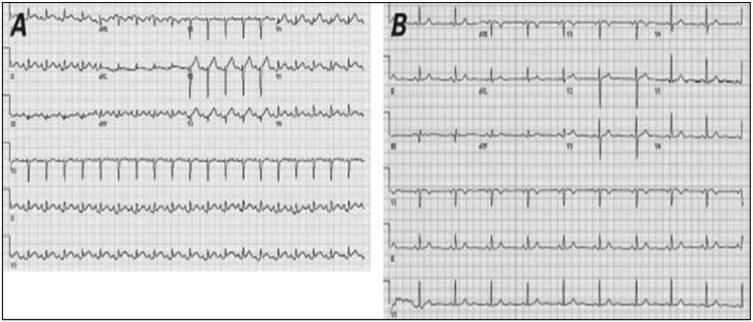
Background and objectives: Currently, there are no specific diagnostic electrocardiogram (ECG) signs for Takotsubo syndrome (TTS) to differentiate it from acute coronary syndromes (ACS). Myocardial oedema has been detected by cardiac magnetic resonance imaging in patients with TTS. Recently it has been postulated that myocardial oedema may be the cause of low QRS voltage (LQRSV) in the admission ECG and attenuation of the amplitude of the QRS complexes (AAQRS) in serial ECGs, noted in a few published cases of patients with TTS. The objective of this study was to evaluate whether the admission ECG of patients with documented TTS reveals LQRSV and whether AAQRS is found when serial ECGs are compared in such patients.
Methods: This study evaluated the prevalence of LQRSV in the admission ECG and AAQRS in serial ECGs in patients with TTS. ECGs of 368 patients with TTS from published reports in the international literature were evaluated for LQRSV (≤5 mm in limb leads and/or ≤10 mm in precordial leads) and AAQRS in serial ECGs.
Results: LQRSV was seen in 91.5% of 200 patients with TTS and one ECG, with a distribution of 49.0, 42.8, 51.0, 52.0, and 46.9%, in lead aVR, and inferior, anterior, lateral, and high lateral ECG lead groups, respectively. AAQRS was seen in 93.5% of 168 patients with TTS and two or more ECGs, with a distribution of 78.3, 74.5, 60.1, 70.7, and 74.5% in lead aVR, and inferior, anterior, lateral, and high lateral ECG lead groups, respectively.
Conclusions: LQRSV and AAQRS are highly prevalent ECG signs in patients with TTS, and should be useful in aiding in its diagnosis and differentiation from ACS, on first contact with the patient on admission to the hospital, and the ensuing 24 hours, in conjunction with echocardiography and coronary arteriography.
Keywords: Attenuation of the QRS complexes; Takotsubo syndrome; cardiac magnetic resonance imaging; diagnosis; electrocardiogram; low ECG QRS voltage; myocardial oedema.
Conflict of interest statement
Figures

References
-
- Jeremy R. Neurogenic heart disease: from Voodoo to Tako-tsubo. Heart Lung Circ 2010; 19: 61–62 - PubMed
-
- Sato H, Tateishi H, Uchida T, et al. Takotsubo-like left ventricular dysfunction due to multivessel coronary spazm. In: Kodama K, Haze K, Hon M. (eds) Clinical aspect of myocardial injury: from ischemia to heart failure. Tokyo: Kagakuhyouronsya, 1990. pp. 56–64
-
- Dote K, Sato H, Tateishi H, et al. Myocardial stunning due to simultaneous multivessel coronary spasms: a review of 5 cases. J Cardiol 1991; 21: 203–214 - PubMed
-
- Ogura R, Hiasa Y, Takahashi T, et al. Specific findings of the standard 12-lead ECG in patients with ‘Takotsubo’ cardiomyopathy: comparison with the findings of acute anterior myocardial infarction. Circ J 2003; 67: 687–690 - PubMed
-
- Inoue M, Shimizu M, Ino H, et al. Differentiation between patients with takotsubo cardiomyopathy and those with anterior acute myocardial infarction. Circ J 2005; 69: 89–94 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
