

Intraprocedural contrast-enhanced ultrasound (CEUS) in liver percutaneous radiofrequency ablation: clinical impact and health technology assessment
- PMID: 24563244
- PMCID: PMC3999370
- DOI: 10.1007/s13244-014-0315-7
Intraprocedural contrast-enhanced ultrasound (CEUS) in liver percutaneous radiofrequency ablation: clinical impact and health technology assessment
Abstract
Objectives: To assess the clinical and the economic impacts of intraprocedural use of contrast-enhanced ultrasound (CEUS) in patients undergoing percutaneous radiofrequency ablation for small (<2.5 cm) hepatocellular carcinomas.
Methods: One hundred and forty-eight hepatocellular carcinomas in 93 patients were treated by percutaneous radiofrequency ablation and immediate assessment by intraprocedural CEUS. Clinical impact, cost effectiveness, and budget, organisational and equity impacts were evaluated and compared with standard treatment without intraprocedural CEUS using the health technology assessment approach.
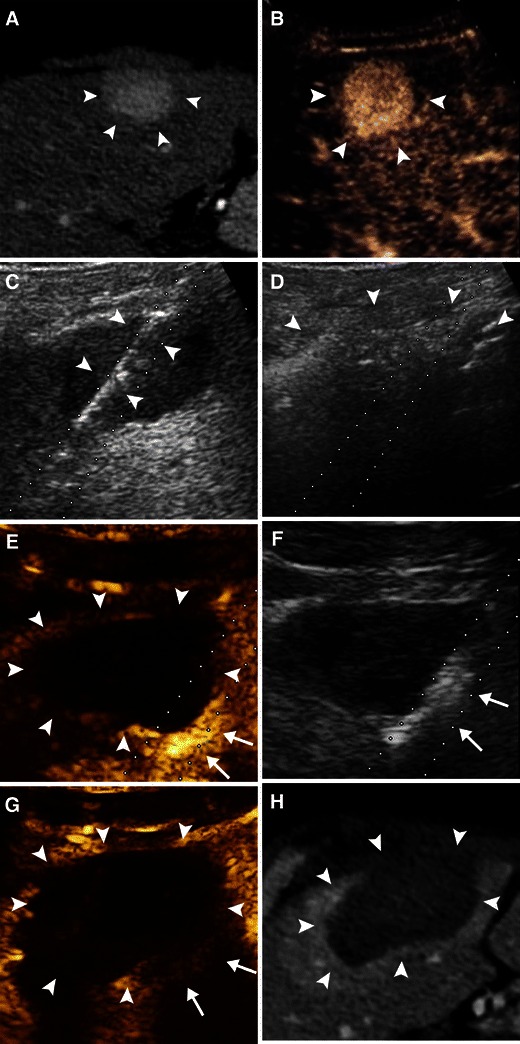
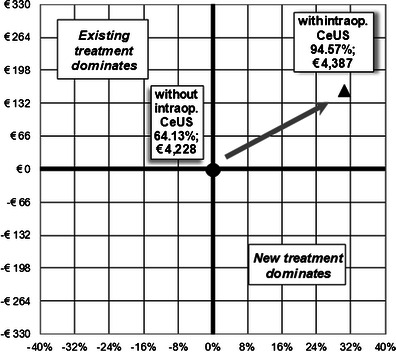
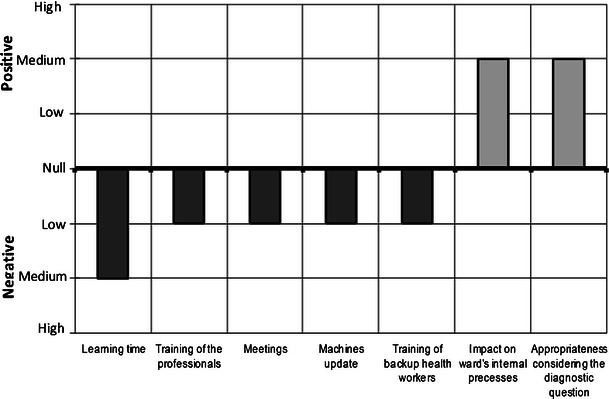
Results: Intraprocedural CEUS detected incomplete ablation in 34/93 (36.5 %) patients, who underwent additional treatment during the same session. At 24-h, complete ablation was found in 88/93 (94.6 %) patients. Thus, a second session of treatment was spared in 29/93 (31.1 %) patients. Cost-effectiveness analysis revealed an advantage for the use of intraprocedural CEUS in comparison with standard treatment (4,639 vs 6,592) with a 21.9 % reduction of the costs to treat the whole sample. Cost per patient for complete treatment was <euro> 4,609 versus <euro> 5,872 respectively. The introduction of intraprocedural CEUS resulted in a low organisational impact, and in a positive impact on equity
Conclusions: Intraprocedural use of CEUS has a relevant clinical impact, reducing the number of re-treatments and the related costs per patient.
Teaching points: • CEUS allows to immediately asses the result of ablation. • Intraprocedural CEUS decreases the number of second ablative sessions. • Intraprocedural CEUS may reduce cost per patient for complete treatment. • Use of intraprocedural CEUS may reduce hospital budget. • Its introduction has low organisational impact, and relevant impact on equity.
Figures

Similar articles
-
Use of intra-procedural fusion imaging combining contrast-enhanced ultrasound using a perflubutane-based contrast agent and auto sweep three-dimensional ultrasound for guiding radiofrequency ablation and evaluating its efficacy in patients with hepatocellular carcinoma.Int J Hyperthermia. 2020;37(1):202-211. doi: 10.1080/02656736.2020.1729422. Int J Hyperthermia. 2020. PMID: 32070164
-
Intraprocedural contrast-enhanced ultrasound-CT/MR fusion imaging assessment in HCC thermal ablation to reduce local tumor progression: compared with routine contrast-enhanced ultrasound.Int J Hyperthermia. 2019;36(1):785-793. doi: 10.1080/02656736.2019.1640899. Int J Hyperthermia. 2019. PMID: 31431086 Clinical Trial.
-
Contrast-enhanced ultrasound improves real-time imaging of ablation region during radiofrequency ablation: preliminary results.Clin Hemorheol Microcirc. 2011;49(1-4):43-54. doi: 10.3233/CH-2011-1456. Clin Hemorheol Microcirc. 2011. PMID: 22214677 Clinical Trial.
-
Radiofrequency ablation for hepatocellular carcinoma: utility of conventional ultrasound and contrast-enhanced ultrasound in guiding and assessing early therapeutic response and short-term follow-up results.Ultrasound Med Biol. 2015 Sep;41(9):2400-11. doi: 10.1016/j.ultrasmedbio.2015.05.004. Epub 2015 Jun 6. Ultrasound Med Biol. 2015. PMID: 26055968 Clinical Trial.
-
Early-stage hepatocellular carcinoma: the high accuracy of real-time contrast-enhanced ultrasonography in the assessment of response to percutaneous treatment.Eur Radiol. 2007 Dec;17 Suppl 6:F80-8. doi: 10.1007/s10406-007-0232-7. Eur Radiol. 2007. PMID: 18376461 Review.
Cited by
-
Contrast Agents for Hepatocellular Carcinoma Imaging: Value and Progression.Front Oncol. 2022 Jun 2;12:921667. doi: 10.3389/fonc.2022.921667. eCollection 2022. Front Oncol. 2022. PMID: 35720001 Free PMC article. Review.
-
Contrast-enhanced ultrasound (CEUS) in HCC diagnosis and assessment of tumor response to locoregional therapies.Abdom Radiol (NY). 2021 Aug;46(8):3579-3595. doi: 10.1007/s00261-021-03059-y. Epub 2021 Apr 7. Abdom Radiol (NY). 2021. PMID: 33825927 Free PMC article. Review.
-
Focal liver lesions in cirrhosis: Role of contrast-enhanced ultrasonography.World J Radiol. 2022 Apr 28;14(4):70-81. doi: 10.4329/wjr.v14.i4.70. World J Radiol. 2022. PMID: 35646291 Free PMC article. Review.
-
Contrast-enhanced ultrasound to ultrasound fusion during microwave ablation: feasibility study in a perfused porcine liver model.J Ultrasound. 2019 Sep;22(3):323-335. doi: 10.1007/s40477-019-00366-5. Epub 2019 Feb 27. J Ultrasound. 2019. PMID: 30811016 Free PMC article.
-
Pancreatic cancer: Does it work if EUS and laser ablation get married?Endosc Ultrasound. 2018 May-Jun;7(3):207-209. doi: 10.4103/eus.eus_28_17. Endosc Ultrasound. 2018. PMID: 29749351 Free PMC article. No abstract available.
References
-
- Cho YK, Rhim H, Noh S. Radiofrequency ablation versus surgical resection as primary treatment of hepatocellular carcinoma meeting the Milan criteria: a systematic review. J Gastroenterol Hepatol. 2011;26:1354–1360. - PubMed
-
- Livraghi T, Meloni F, Di Stasi M, Rolle E, Solbiati L, Tinelli C, et al. Sustained complete response and complications rates after radiofrequency ablation of very early hepatocellular carcinoma in cirrhosis: is resection still the treatment of choice? Hepatology. 2008;47:82–89. doi: 10.1002/hep.21933. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
