

Leaving tissue associated with infrequent intracranial EEG seizure onsets is compatible with post-operative seizure freedom
- PMID: 24563805
- PMCID: PMC3930198
- DOI: 10.3233/PEP-12033
Leaving tissue associated with infrequent intracranial EEG seizure onsets is compatible with post-operative seizure freedom
Abstract
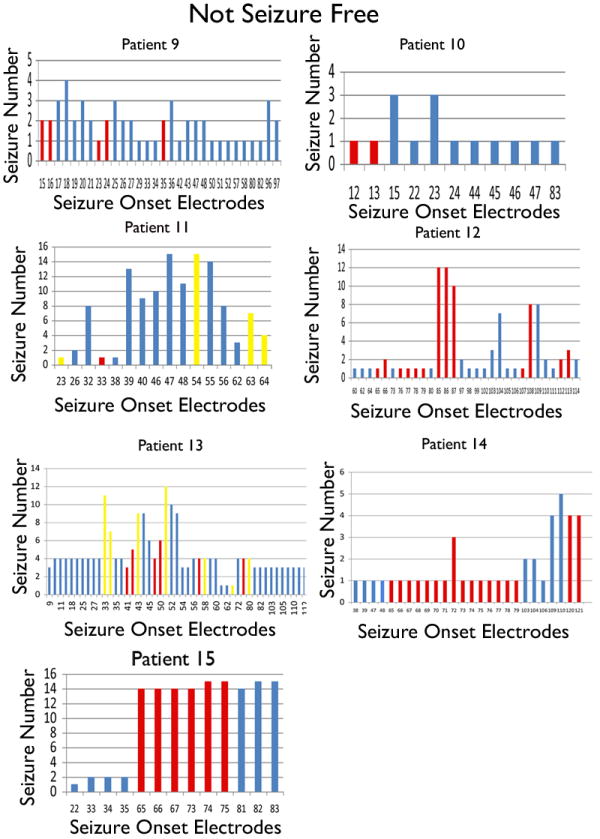
Identify seizure onset electrodes that need to be resected for seizure freedom in children undergoing intracranial electroencephalography recording for treatment of medically refractory epilepsy. All children undergoing intracranial electroencephalography subdural grid electrode placement at the Children's Hospital of Philadelphia from 2002-2008 were asked to enroll. We utilized intraoperative pictures to determine the location of the electrodes and define the resection cavity. A total of 15 patients had surgical fields that allowed for complete identification of the electrodes over the area of resection. Eight of 15 patients were seizure free after a follow up of 1.7 to 8 yr. Only one seizure-free patient had complete resection of all seizure onset associated tissue. Seizure free patients had resection of 64.1% of the seizure onset electrode associated tissue, compared to 35.2% in the not seizure free patients (p=0.05). Resection of tissue associated with infrequent seizure onsets did not appear to be important for seizure freedom. Resecting ≥ 90% of the electrodes from the predominant seizure contacts predicted post-operative seizure freedom (p=0.007). The best predictor of seizure freedom was resecting ≥ 90% of tissue involved in majority of a patient's seizures. Resection of tissue under infrequent seizure onset electrodes was not necessary for seizure freedom.
Keywords: Epilepsy; cortical dysplasia; epilepsy surgery; intracranial electroencephalography; neocortical epilepsy.
Conflict of interest statement
Disclosures: Drs. Marsh, Ziskind, Celix, Storm and Porter have no conflict of interest to report. Mr. Huang and Peltzer have no conflict of interest to report.
Figures


Similar articles
-
MEG predicts outcome following surgery for intractable epilepsy in children with normal or nonfocal MRI findings.Epilepsia. 2007 Jan;48(1):149-57. doi: 10.1111/j.1528-1167.2006.00901.x. Epilepsia. 2007. PMID: 17241222
-
Medically resistant pediatric insular-opercular/perisylvian epilepsy. Part 2: outcome following resective surgery.J Neurosurg Pediatr. 2016 Nov;18(5):523-535. doi: 10.3171/2016.4.PEDS15618. Epub 2016 Jul 29. J Neurosurg Pediatr. 2016. PMID: 27472665
-
Localization yield and seizure outcome in patients undergoing bilateral SEEG exploration.Epilepsia. 2019 Jan;60(1):107-120. doi: 10.1111/epi.14624. Epub 2018 Dec 26. Epilepsia. 2019. PMID: 30588603 Free PMC article.
-
Seizure outcome following primary motor cortex-sparing resective surgery for perirolandic focal cortical dysplasia.Int J Surg. 2016 Dec;36(Pt B):466-476. doi: 10.1016/j.ijsu.2015.10.036. Epub 2015 Nov 2. Int J Surg. 2016. PMID: 26542986 Review.
-
Patient phenotypes and clinical outcomes in invasive monitoring for epilepsy: An individual patient data meta-analysis.Epilepsy Behav. 2020 Jan;102:106652. doi: 10.1016/j.yebeh.2019.106652. Epub 2019 Nov 23. Epilepsy Behav. 2020. PMID: 31770717 Review.
Cited by
-
Co-activation of interictal epileptiform discharges localizes seizure onset zone and fluctuates with brain state.Brain Commun. 2025 Apr 3;7(2):fcaf127. doi: 10.1093/braincomms/fcaf127. eCollection 2025. Brain Commun. 2025. PMID: 40212342 Free PMC article.
-
Spatiotemporal Mapping of Interictal Spike Propagation: A Novel Methodology Applied to Pediatric Intracranial EEG Recordings.Front Neurol. 2016 Dec 19;7:229. doi: 10.3389/fneur.2016.00229. eCollection 2016. Front Neurol. 2016. PMID: 28066315 Free PMC article.
-
Evaluating resective surgery targets in epilepsy patients: A comparison of quantitative EEG methods.J Neurosci Methods. 2018 Jul 15;305:54-66. doi: 10.1016/j.jneumeth.2018.04.021. Epub 2018 May 18. J Neurosci Methods. 2018. PMID: 29753683 Free PMC article.
-
Prognostic application of lesion network mapping to epilepsy surgery outcomes in pediatric tuberous sclerosis complex.Epilepsia. 2025 Jun;66(6):1854-1864. doi: 10.1111/epi.18320. Epub 2025 Mar 5. Epilepsia. 2025. PMID: 40042434 Free PMC article.
-
High frequency oscillation network dynamics predict outcome in non-palliative epilepsy surgery.Brain Commun. 2024 Feb 7;6(1):fcae032. doi: 10.1093/braincomms/fcae032. eCollection 2024. Brain Commun. 2024. PMID: 38384998 Free PMC article.
References
-
- Lüders HO, Najm I, Nair D, Widdess-Walsh P, Bingman W. The epileptogenic zone: general principles. Epileptic Disord. 2006;8(Suppl 2):S1–S9. - PubMed
-
- Krsek P, Maton B, Jayakar P, Dean P, Korman B, Rey G, et al. Incomplete resection of focal cortical dysplasia is the main predictor of poor postsurgical outcome. Neurology. 2009;72(3):217–23. - PubMed
-
- Jayakar P, Dunoyer C, Dean P, Ragheb J, Resnick T, Morrison G, et al. Epilepsy surgery in patients with normal or nonfocal MRI scans: integrative strategies offer long-term seizure relief. Epilepsia. 2008;49(5):758–64. - PubMed
-
- Paolicchi JM, Jayakar P, Dean P, Yaylali I, Morrison G, Prats A, et al. Predictors of outcome in pediatric epilepsy surgery. Neurology. 2000;54(3):642–7. - PubMed
-
- Hader WJ, Mackay M, Otsubo H, Chitoku S, Weiss S, Becker L, et al. Cortical dysplastic lesions in children with intractable epilepsy: role of complete resection. J Neurosurg. 2004;100(2 Suppl):110–7. Pediatrics. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources