

Financial incentives and coverage of child health interventions: a systematic review and meta-analysis
- PMID: 24564520
- PMCID: PMC3847540
- DOI: 10.1186/1471-2458-13-S3-S30
Financial incentives and coverage of child health interventions: a systematic review and meta-analysis
Abstract
Background: Financial incentives are widely used strategies to alleviate poverty, foster development, and improve health. Cash transfer programs, microcredit, user fee removal policies and voucher schemes that provide direct or indirect monetary incentives to households have been used for decades in Latin America, Sub-Saharan Africa, and more recently in Southeast Asia. Until now, no systematic review of the impact of financial incentives on coverage and uptake of health interventions targeting children under 5 years of age has been conducted. The objective of this review is to provide estimates on the effect of six types of financial incentive programs: (i) Unconditional cash transfers (CT), (ii) Conditional cash transfers (CCT), (iii) Microcredit (MC), (iv) Conditional Microcredit (CMC), (v) Voucher schemes (VS) and (vi) User fee removal (UFR) on the uptake and coverage of health interventions targeting children under the age of five years.
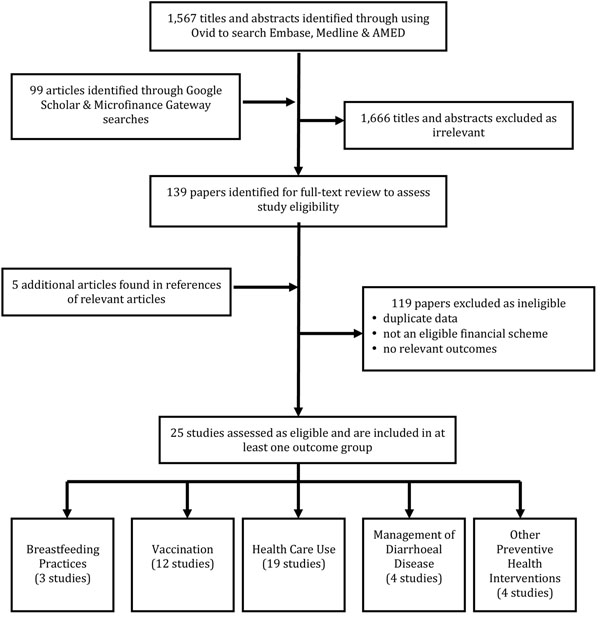
Methods: We conducted systematic searches of a series of databases until September 1st, 2012, to identify relevant studies reporting on the impact of financial incentives on coverage of health interventions and behaviors targeting children under 5 years of age. The quality of the studies was assessed using the CHERG criteria. Meta-analyses were undertaken to estimate the effect when multiple studies meeting our inclusion criteria were available.
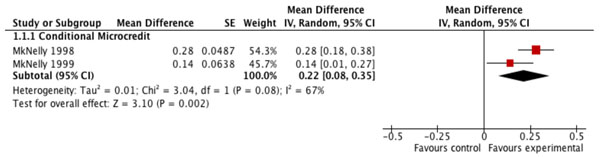
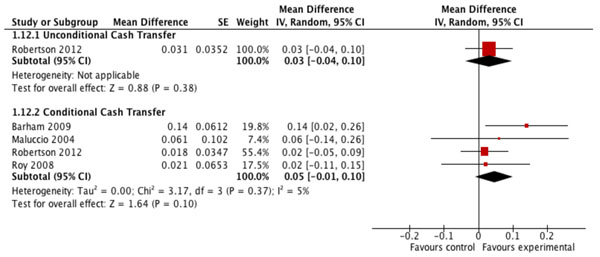
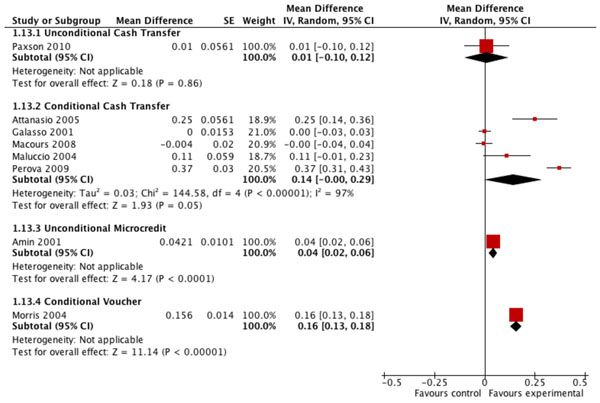
Results: Our searches resulted in 1671 titles identified 25 studies reporting on the impact of financial incentive programs on 5 groups of coverage indicators: breastfeeding practices (breastfeeding incidence, proportion of children receiving colostrum and early initiation of breastfeeding, exclusive breastfeeding for six months and duration of breastfeeding); vaccination (coverage of full immunization, partial immunization and specific antigens); health care use (seeking healthcare when child was ill, visits to health facilities for preventive reasons, visits to health facilities for any reason, visits for health check-up including growth control); management of diarrhoeal disease (ORS use during diarrhea episode, continued feeding during diarrhea, healthcare during diarrhea episode) and other preventive health interventions (iron supplementation, vitamin A, zinc supplementation, preventive deworming). The quality of evidence on the effect of financial incentives on breastfeeding practices was low but seems to indicate a potential positive impact on receiving colostrum, early initiation of breastfeeding, exclusive breastfeeding and mean duration of exclusive breastfeeding. There is no effect of financial incentives on immunization coverage although there was moderate quality evidence of conditional cash transfers leading to a small but non-significant increase in coverage of age-appropriate immunization. There was low quality evidence of impact of CCT on healthcare use by children under age 5 (Risk difference: 0.14 [95%CI: 0.03; 0.26]) as well as low quality evidence of an effect of user fee removal on use of curative health services (RD=0.62 [0.41; 0.82]).
Conclusions: Financial incentives may have potential to promote increased coverage of several important child health interventions, but the quality of evidence available is low. The more pronounced effects seem to be achieved by programs that directly removed user fees for access to health services. Some indication of effect were also observed for programs that conditioned financial incentives on participation in health education and attendance to health care visits. This finding suggest that the measured effect may be less a consequence of the financial incentive and more due to conditionalities addressing important informational barriers.
Figures
References
-
- World Health Organization. Public health agencies and cash transfer programmes : making the case for greater involvement. Geneva: World Health Organization; 2011.
-
- Gautam Hazarika, B G-K. Household Access to Microcredit and Children’s Food Security in Rural Malawi: A Gender Perspective. 2008. pp. 1–18.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
