

Prenatal antidepressant exposure: clinical and preclinical findings
- PMID: 24567054
- PMCID: PMC3973612
- DOI: 10.1124/pr.111.005207
Prenatal antidepressant exposure: clinical and preclinical findings
Abstract
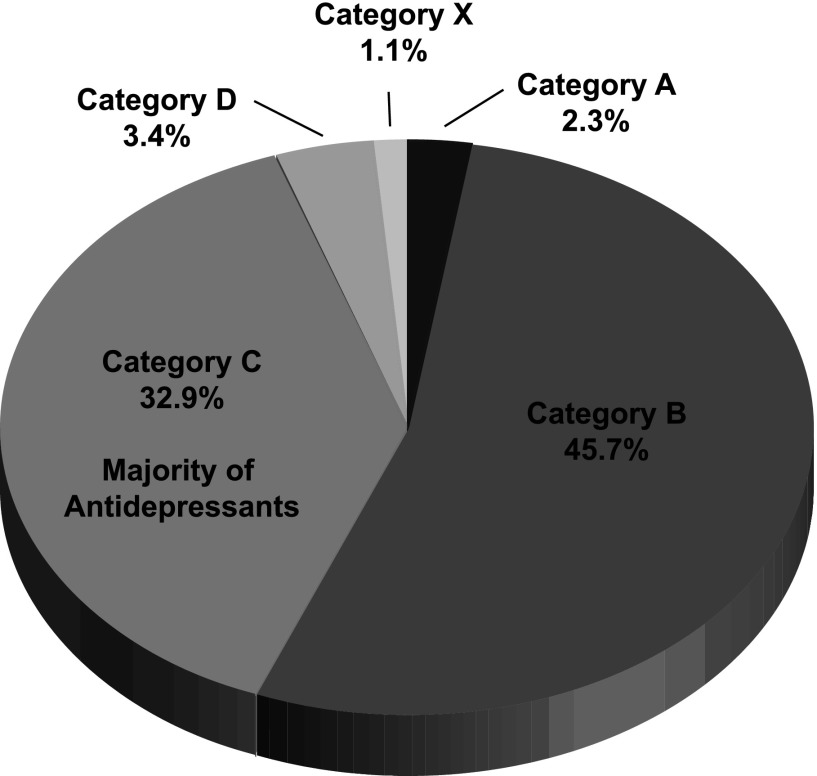
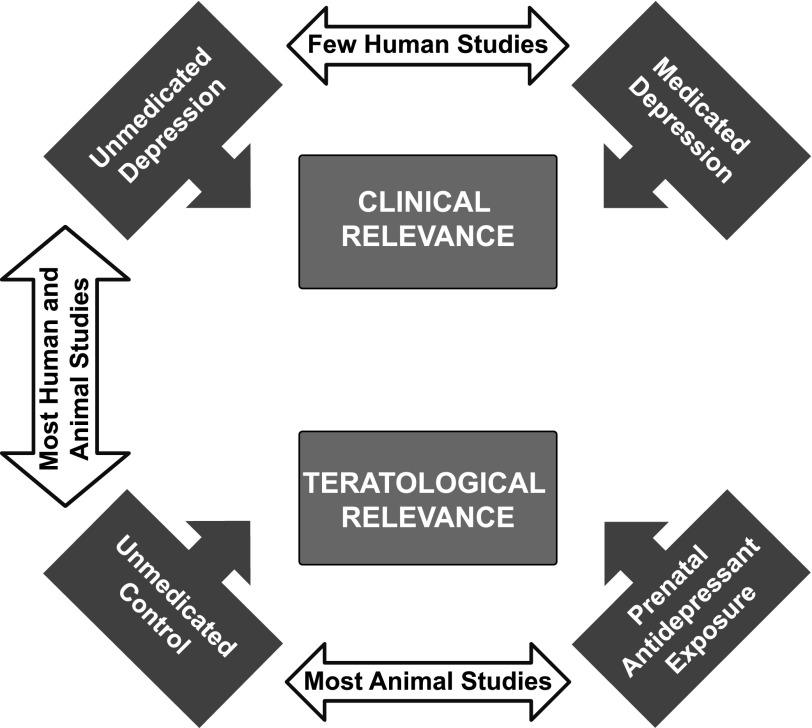
Pharmacological treatment of any maternal illness during pregnancy warrants consideration of the consequences of the illness and/or medication for both the mother and unborn child. In the case of major depressive disorder, which affects up to 10-20% of pregnant women, the deleterious effects of untreated depression on the offspring can be profound and long lasting. Progress has been made in our understanding of the mechanism(s) of action of antidepressants, fetal exposure to these medications, and serotonin's role in development. New technologies and careful study designs have enabled the accurate sampling of maternal serum, breast milk, umbilical cord serum, and infant serum psychotropic medication concentrations to characterize the magnitude of placental transfer and exposure through human breast milk. Despite this progress, the extant clinical literature is largely composed of case series, population-based patient registry data that are reliant on nonobjective means and retrospective recall to determine both medication and maternal depression exposure, and limited inclusion of suitable control groups for maternal depression. Conclusions drawn from such studies often fail to incorporate embryology/neurotransmitter ontogeny, appropriate gestational windows, or a critical discussion of statistically versus clinically significant. Similarly, preclinical studies have predominantly relied on dosing models, leading to exposures that may not be clinically relevant. The elucidation of a defined teratological effect or mechanism, if any, has yet to be conclusively demonstrated. The extant literature indicates that, in many cases, the benefits of antidepressant use during pregnancy for a depressed pregnant woman may outweigh potential risks.
Figures
Similar articles
-
[Current evaluation of teratogenic and fetotoxic effects of psychotropic drugs].Seishin Shinkeigaku Zasshi. 2014;116(12):996-1004. Seishin Shinkeigaku Zasshi. 2014. PMID: 25823351 Review. Japanese.
-
Prenatal antidepressant exposure and child behavioural outcomes at 7 years of age: a study within the Danish National Birth Cohort.BJOG. 2016 Nov;123(12):1919-1928. doi: 10.1111/1471-0528.13611. Epub 2015 Sep 15. BJOG. 2016. PMID: 26374344
-
Prenatal exposure to escitalopram and/or stress in rats produces limited effects on endocrine, behavioral, or gene expression measures in adult male rats.Neurotoxicol Teratol. 2013 Sep-Oct;39:100-9. doi: 10.1016/j.ntt.2013.07.008. Epub 2013 Jul 30. Neurotoxicol Teratol. 2013. PMID: 23906943 Free PMC article.
-
Acute and long-term behavioral outcome of infants and children exposed in utero to either maternal depression or antidepressants: a review of the literature.J Clin Psychiatry. 2014 Oct;75(10):e1142-52. doi: 10.4088/JCP.13r08926. J Clin Psychiatry. 2014. PMID: 25373125 Review.
-
Association of Antidepressant Medication Use During Pregnancy With Intellectual Disability in Offspring.JAMA Psychiatry. 2017 Oct 1;74(10):1031-1038. doi: 10.1001/jamapsychiatry.2017.1727. JAMA Psychiatry. 2017. PMID: 28700807 Free PMC article.
Cited by
-
Cell-Based High-Throughput Screening for Aromatase Inhibitors in the Tox21 10K Library.Toxicol Sci. 2015 Oct;147(2):446-57. doi: 10.1093/toxsci/kfv141. Epub 2015 Jul 3. Toxicol Sci. 2015. PMID: 26141389 Free PMC article.
-
Prenatal exposure to psychotropics and analgesics on cognitive, linguistic and educational outcomes - a scoping review with focus on validity and reliability of outcome measures.BMC Pregnancy Childbirth. 2025 Mar 3;25(1):234. doi: 10.1186/s12884-025-07235-6. BMC Pregnancy Childbirth. 2025. PMID: 40033241 Free PMC article.
-
Prenatal stress, regardless of concurrent escitalopram treatment, alters behavior and amygdala gene expression of adolescent female rats.Neuropharmacology. 2015 Oct;97:251-8. doi: 10.1016/j.neuropharm.2015.05.012. Epub 2015 May 30. Neuropharmacology. 2015. PMID: 26032436 Free PMC article.
-
Imipramine and Venlafaxine Differentially Affect Primary Glial Cultures of Prenatally Stressed Rats.Front Pharmacol. 2020 Jan 31;10:1687. doi: 10.3389/fphar.2019.01687. eCollection 2019. Front Pharmacol. 2020. PMID: 32076407 Free PMC article.
-
Prenatal and early postnatal measures of brain development and childhood sleep patterns.Pediatr Res. 2018 Apr;83(4):760-766. doi: 10.1038/pr.2017.318. Epub 2018 Jan 17. Pediatr Res. 2018. PMID: 29244799
References
-
- ACOG Committee on Practice Bulletins–Obstetrics (2008) ACOG Practice Bulletin: Clinical management guidelines for obstetrician-gynecologists number 92, April 2008 (replaces practice bulletin number 87, November 2007). Use of psychiatric medications during pregnancy and lactation. Obstet Gynecol 111:1001–1020 - PubMed
-
- Addis A, Koren G. (2000) Safety of fluoxetine during the first trimester of pregnancy: a meta-analytical review of epidemiological studies. Psychol Med 30:89–94 - PubMed
-
- Ali SF, Buelke-Sam J, Newport GD, Slikker W., Jr (1986) Early neurobehavioral and neurochemical alterations in rats prenatally exposed to imipramine. Neurotoxicology 7:365–380 - PubMed
-
- Als H, Tronick E, Lester BM, Brazelton TB. (1977) The Brazelton Neonatal Behavioral Assessment Scale (BNBAS). J Abnorm Child Psychol 5:215–231 - PubMed
-
- Altshuler LL, Burt VK, McMullen M, Hendrick V. (1995) Breastfeeding and sertraline: a 24-hour analysis. J Clin Psychiatry 56:243–245 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
