

National hospice survey results: for-profit status, community engagement, and service
- PMID: 24567076
- PMCID: PMC4315613
- DOI: 10.1001/jamainternmed.2014.3
National hospice survey results: for-profit status, community engagement, and service
Abstract
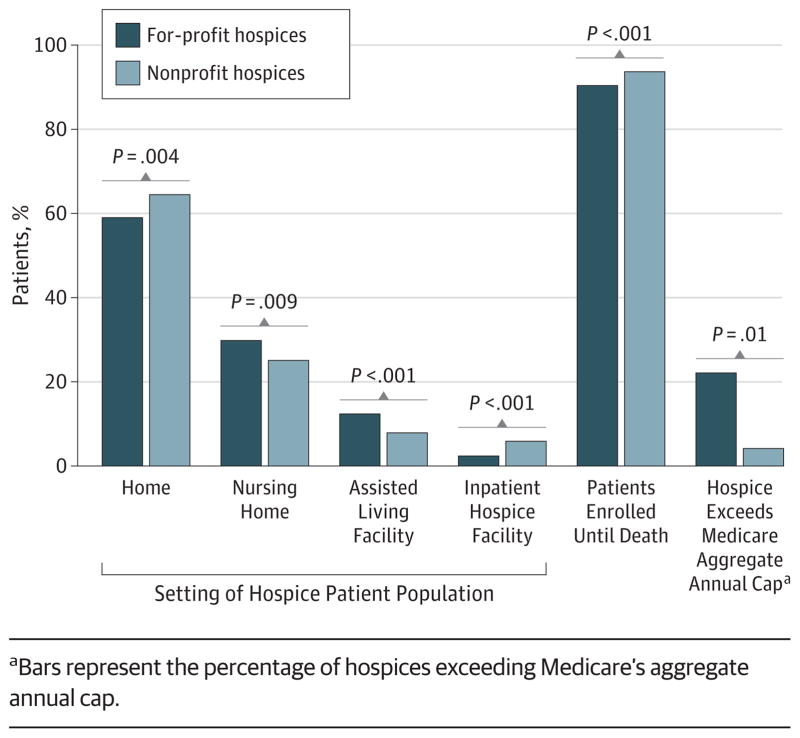
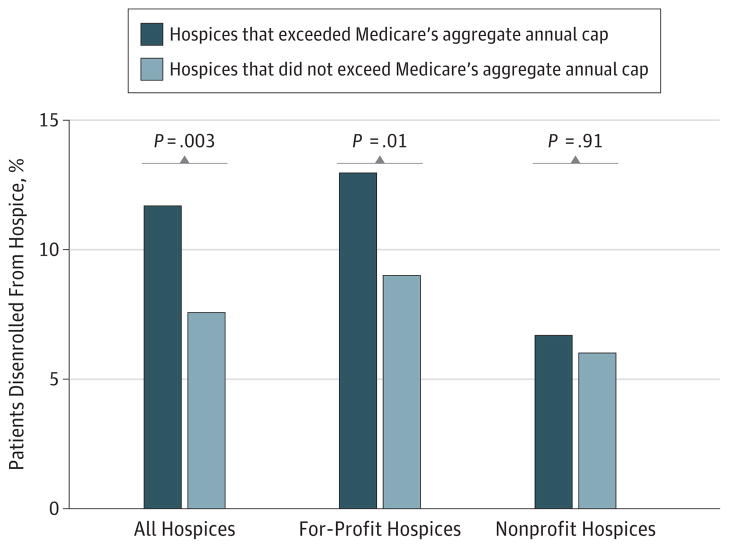
IMPORTANCE The impact of the substantial growth in for-profit hospices in the United States on quality and hospice access has been intensely debated, yet little is known about how for-profit and nonprofit hospices differ in activities beyond service delivery. OBJECTIVE To determine the association between hospice ownership and (1) provision of community benefits, (2) setting and timing of the hospice population served, and (3) community outreach. DESIGN, SETTING, AND PARTICIPANTS Cross-sectional survey (the National Hospice Survey), conducted from September 2008 through November 2009, of a national random sample of 591 Medicare-certified hospices operating throughout the United States. EXPOSURES For-profit or nonprofit hospice ownership. MAIN OUTCOMES AND MEASURES Provision of community benefits; setting and timing of the hospice population served; and community outreach. RESULTS A total of 591 hospices completed our survey (84% response rate). For-profit hospices were less likely than nonprofit hospices to provide community benefits including serving as training sites (55% vs 82%; adjusted relative risk [ARR], 0.67 [95% CI, 0.59-0.76]), conducting research (18% vs 23%; ARR, 0.67 [95% CI, 0.46-0.99]), and providing charity care (80% vs 82%; ARR, 0.88 [95% CI, 0.80-0.96]). For-profit compared with nonprofit hospices cared for a larger proportion of patients with longer expected hospice stays including those in nursing homes (30% vs 25%; P = .009). For-profit hospices were more likely to exceed Medicare's aggregate annual cap (22% vs 4%; ARR, 3.66 [95% CI, 2.02-6.63]) and had a higher patient disenrollment rate (10% vs 6%; P < .001). For-profit were more likely than nonprofit hospices to engage in outreach to low-income communities (61% vs 46%; ARR, 1.23 [95% CI, 1.05-1.44]) and minority communities (59% vs 48%; ARR, 1.18 [95% CI, 1.02-1.38]) and less likely to partner with oncology centers (25% vs 33%; ARR, 0.59 [95% CI, 0.44-0.80]). CONCLUSIONS AND RELEVANCE Ownership-related differences are apparent among hospices in community benefits, population served, and community outreach. Although Medicare's aggregate annual cap may curb the incentive to focus on long-stay hospice patients, additional regulatory measures such as public reporting of hospice disenrollment rates should be considered as the share of for-profit hospices in the United States continues to increase.
Conflict of interest statement
Figures
Comment in
-
The changing face of the hospice industry: what really matters?JAMA Intern Med. 2014 Apr;174(4):507-8. doi: 10.1001/jamainternmed.2013.13304. JAMA Intern Med. 2014. PMID: 24566818 No abstract available.
Similar articles
-
Association of hospice agency profit status with patient diagnosis, location of care, and length of stay.JAMA. 2011 Feb 2;305(5):472-9. doi: 10.1001/jama.2011.70. JAMA. 2011. PMID: 21285424 Free PMC article.
-
Factors Associated With Hospices' Nonparticipation in Medicare's Hospice Compare Public Reporting Program.Med Care. 2019 Jan;57(1):28-35. doi: 10.1097/MLR.0000000000001016. Med Care. 2019. PMID: 30489545
-
Ownership status and patterns of care in hospice: results from the National Home and Hospice Care Survey.Med Care. 2004 May;42(5):432-8. doi: 10.1097/01.mlr.0000124246.86156.54. Med Care. 2004. PMID: 15083103
-
Nonprofit conversion: theory, evidence, and state policy options.Health Serv Res. 1998 Dec;33(5 Pt 2):1495-535. Health Serv Res. 1998. PMID: 9865231 Free PMC article. Review.
-
Charity and community: the role of nonprofit ownership in a managed health care system.J Health Polit Policy Law. 1996 Winter;21(4):697-751. doi: 10.1215/03616878-21-4-697. J Health Polit Policy Law. 1996. PMID: 8892004 Review.
Cited by
-
Hospice Quality, Race, and Disenrollment in Hospice Enrollees With Dementia.J Palliat Med. 2023 Aug;26(8):1100-1108. doi: 10.1089/jpm.2023.0011. Epub 2023 Apr 3. J Palliat Med. 2023. PMID: 37010377 Free PMC article.
-
Massage, Music, and Art Therapy in Hospice: Results of a National Survey.J Pain Symptom Manage. 2015 Jun;49(6):1035-41. doi: 10.1016/j.jpainsymman.2014.11.295. Epub 2014 Dec 30. J Pain Symptom Manage. 2015. PMID: 25555445 Free PMC article.
-
Continuous Home Care Reduces Hospice Disenrollment and Hospitalization After Hospice Enrollment.J Pain Symptom Manage. 2016 Dec;52(6):813-821. doi: 10.1016/j.jpainsymman.2016.05.031. Epub 2016 Sep 30. J Pain Symptom Manage. 2016. PMID: 27697564 Free PMC article.
-
Has Hospice Use Changed? 2000-2010 Utilization Patterns.Med Care. 2015 Jan;53(1):95-101. doi: 10.1097/MLR.0000000000000256. Med Care. 2015. PMID: 25373406 Free PMC article.
-
In Search of Hospice Information: Consumer Information Available on Hospice Compare and Yelp.Palliat Med Rep. 2020 Apr 30;1(1):18-24. doi: 10.1089/pmr.2020.0022. eCollection 2020. Palliat Med Rep. 2020. PMID: 34223451 Free PMC article.
References
-
- National Hospice and Palliative Care Organization. [Accessed February 2012];NHPCO Facts and Figures: Hospice Care in America. 2011 http://www.nhpco.org/sites/default/files/public/Statistics_Research/2011....
-
- Medicare Payment Advisory Commission. Report to the Congress: Medicare Beneficiaries’ Access to Hospice. Washington, DC: Medicare Payment Advisory Commission; 2002.
-
- Medicare Payment Advisory Commission. Report to the Congress: Reforming the Delivery System. Washington, DC: Medicare Payment Advisory Commission; 2008. pp. 203–240.
-
- Medicare Payment Advisory Commission. Report to the Congress: Medicare’s Payment Policy: Reforming Medicare’s Hospice Benefit. Washington, DC: Medicare Payment Advisory Commission; 2009.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
