

Muscle motor point identification is essential for optimizing neuromuscular electrical stimulation use
- PMID: 24568180
- PMCID: PMC3938308
- DOI: 10.1186/1743-0003-11-17
Muscle motor point identification is essential for optimizing neuromuscular electrical stimulation use
Abstract
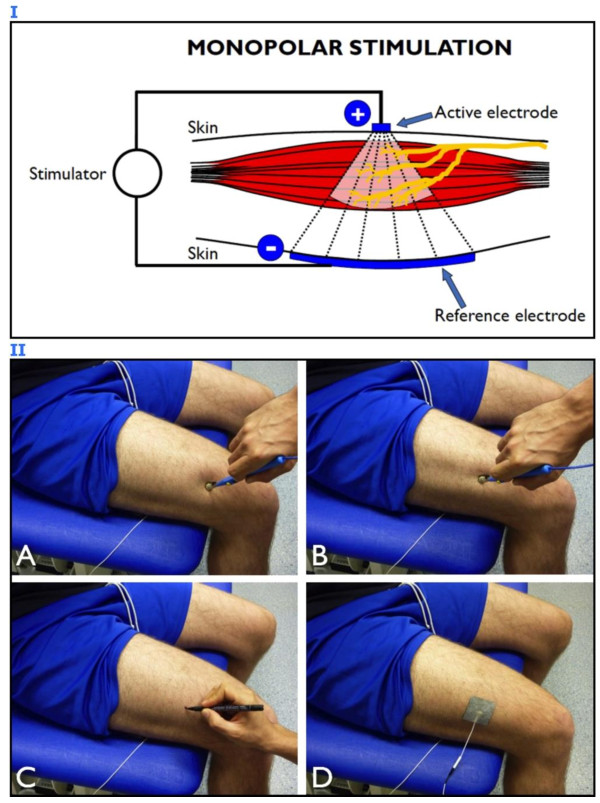
Transcutaneous neuromuscular electrical stimulation applied in clinical settings is currently characterized by a wide heterogeneity of stimulation protocols and modalities. Practitioners usually refer to anatomic charts (often provided with the user manuals of commercially available stimulators) for electrode positioning, which may lead to inconsistent outcomes, poor tolerance by the patients, and adverse reactions. Recent evidence has highlighted the crucial importance of stimulating over the muscle motor points to improve the effectiveness of neuromuscular electrical stimulation. Nevertheless, the correct electrophysiological definition of muscle motor point and its practical significance are not always fully comprehended by therapists and researchers in the field. The commentary describes a straightforward and quick electrophysiological procedure for muscle motor point identification. It consists in muscle surface mapping by using a stimulation pen-electrode and it is aimed at identifying the skin area above the muscle where the motor threshold is the lowest for a given electrical input, that is the skin area most responsive to electrical stimulation. After the motor point mapping procedure, a proper placement of the stimulation electrode(s) allows neuromuscular electrical stimulation to maximize the evoked tension, while minimizing the dose of the injected current and the level of discomfort. If routinely applied, we expect this procedure to improve both stimulation effectiveness and patient adherence to the treatment.The aims of this clinical commentary are to present an optimized procedure for the application of neuromuscular electrical stimulation and to highlight the clinical implications related to its use.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
