

Guidelines for the prevention and treatment of opportunistic infections in HIV-exposed and HIV-infected children: recommendations from the National Institutes of Health, Centers for Disease Control and Prevention, the HIV Medicine Association of the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the American Academy of Pediatrics
- PMID: 24569199
- PMCID: PMC4169043
- DOI: 10.1097/01.inf.0000437856.09540.11
Guidelines for the prevention and treatment of opportunistic infections in HIV-exposed and HIV-infected children: recommendations from the National Institutes of Health, Centers for Disease Control and Prevention, the HIV Medicine Association of the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the American Academy of Pediatrics
Figures
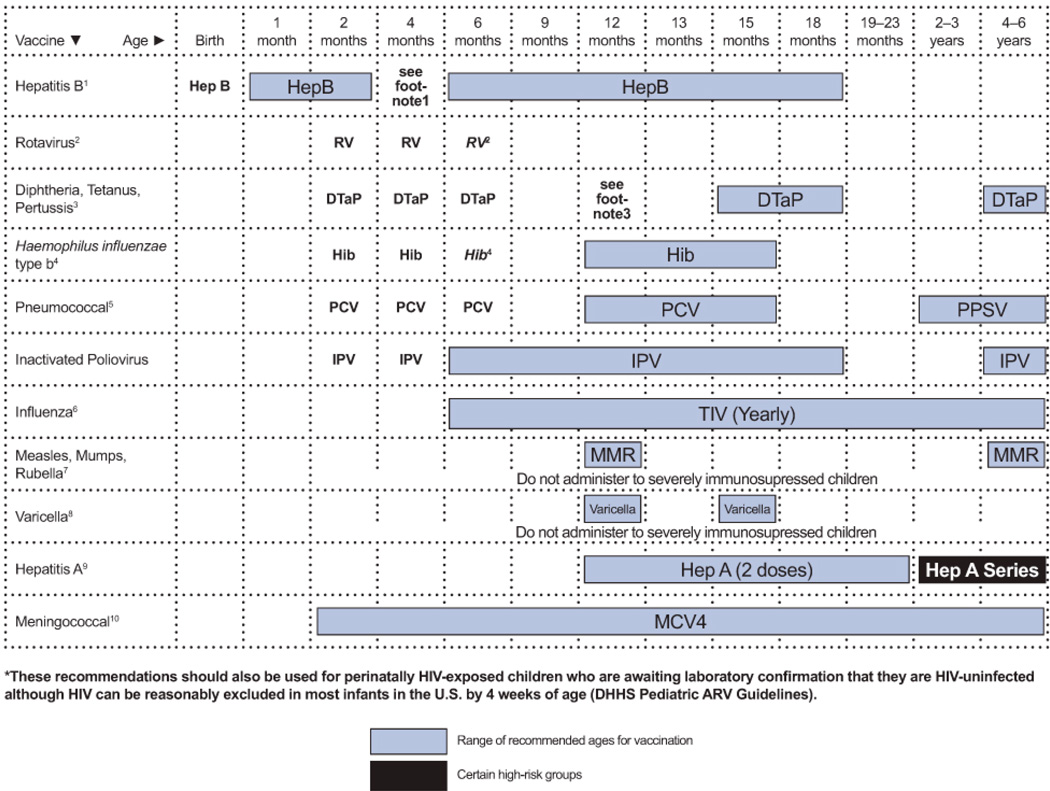
Administer monovalent HepB to all newborns before hospital discharge.
If mother is hepatitis B surface antigen (HBsAg)-positive, administer HepB and 0.5 mL of hepatitis B immune globulin (HBIG) within 12 hours after birth.
If mother’s HBsAg status is unknown, administer HepB within 12 hours after birth. Determine mother’s HBsAg status as soon as possible and if HBsAg-positive, administer HBIG as soon as possible
The HepB series should be completed with either monovalent HepB or a combination vaccine containing HepB. The second dose should be administered at ages 1 through 2 months. Monovalent HepB should be used for doses administered before 6 weeks. The final dose should be administered no earlier than age 24 weeks. Infants who did not receive a birth dose should receive 3 doses of a HepB-containing vaccine on an age-appropriate schedule
It is permissible to administer 4 doses of HepB when combination vaccines are administered after the birth dose. If monovalent HepB is used for doses after the birth dose, a dose at age 4 months is not needed.
Infants born to HBsAg-positive mothers should be tested for HBsAg and the antibody to HBsAg (anti-HBs) after completion of at least 3 doses of a licensed HepB series, at ages 9 through 18 months(generally at the next well-child visit).
Testing is recommended for HIV-infected children and should be performed 1 to 2 months after administration of the last dose of the vaccine series using a method that allows determination of a protective level of anti-HBs (≥10 mIU/mL).
Children with anti-HBs < 10 mIU/mL after the primary schedule should receive a second series, followed by anti-HBs testing 1 to 2 months after the third dose, which usually is more practical than serologic testing after one or more doses of vaccine.
In HIV-infected children, the need for booster doses has not been determined. Annual anti-HBs testing and booster doses when anti-HBs levels decline to < 10 mIU/mL should be considered in individuals with ongoing risk for exposure. See MMWR 2005:54(No. RR-16).
Practitioners should consider the potential risks and benefits of administering rotavirus vaccine to infants with known or suspected altered immunocompetence. Consultation with an immunologist or infectious disease specialist is advised. Limited safety and efficacy data are available for the administration of rotavirus vaccines to infants who are potentially immunocompromised, including those who are HIV-infected. However, the following considerations support vaccination of HIV-exposed or HIV-infected infants:
In infants born to HIV-positive mothers, the HIV diagnosis may not be established before the age of the first rotavirus vaccine dose (only 1.5%–3% of HIV-exposed infants in the United States will eventually be determined to be HIV-infected), and
Vaccine strains of rotavirus are considerably attenuated.
The maximum age for the first dose in the series is 14 weeks and 6 days; for the final dose in the series, it is 8 months and 0 days. Vaccination should not be initiated for infants aged 15 weeks and 0 days or older.
If Rotarix® is administered at ages 2 and 4 months, a dose at 6 months is not indicated.
The fourth dose may be administered as early as age 12 months, provided that at least 6 months have elapsed since the third dose.
If PRP-OMP (PedvaxHIB® or ComVax® [Hep B-Hib]) is administered at ages 2 and 4 months, a dose at age 6 months is not indicated.
Hiberix should not be used for doses at ages 2, 4, or 6 months for the primary series but may be used as the final dose in children aged 12 months through 4 years.
One dose of Hib vaccine should be administered to unvaccinated or partially vaccinated persons aged 5 years or older who have leukemia, malignant neoplasms, anatomic or functional asplenia (including sickle cell disease), HIV infection, or other immunocompromising conditions.
A PCV series begun with 7-valent PCV (PCV7) should be completed with 13-valent PCV (PCV13). A single supplemental dose of PCV13 is recommended for children aged 14 months through 71 months who have received an age-appropriate series of PCV7. For incompletely vaccinated children aged 24 months through 71 months, administer 2 doses of PCV13 at least 8 weeks apart. Children who have previously received 3 PCV doses need only 1 dose.
Children aged 2 years or older also should receive PPSV after their last PCV dose.
Administer annually to HIV-infected children aged 6 months through 6 years and to all their eligible close contacts (including household members). TIV is recommended for HIV-infected children.
For healthy, non-pregnant close contacts aged 2 years through 49 years, either live, attenuated influenza vaccine (LAIV) or TIV may be used.
Children receiving TIV should receive 0.25 mL if aged 6 through 35 months or 0.5 mL if aged 3 years or older.
Administer 2 doses (separated by at least 4 weeks) to children aged younger than 9 years per current influenza vaccine recommendations.
If 4 or more doses are administered prior to age 4 years, an additional dose should be administered at ages 4 through 6 years.
The final dose in the series should be administered on or after the fourth birthday and at least 6 months after the previous dose.
Two doses of MMR vaccine for all HIV-infected individuals aged ≥12 months who do not have evidence of current severe immunosuppression (i.e., individuals aged ≤5 years must have CD4 T lymphocyte [CD4] percentages ≥15% for ≥6 months; and individuals aged >5 years must have CD4 percentages ≥15% and CD4 ≥200 lymphocytes/mm3 for ≥6 months) or other current evidence of measles, rubella, and mumps immunity. In cases when only CD4 cell counts or only CD4 percentages are available for those older than age 5 years, the assessment of severe immunosuppression can be based on the CD4 values (count or percentage) that are available. In cases when CD4 percentages are not available for those aged ≤5 years, the assessment of severe immunosuppression can be based on age-specific CD4 counts at the time CD4 counts were measured; i.e., absence of severe immunosuppression is defined as ≥6 months above age-specific CD4 count criteria: CD4 count >750 lymphocytes/mm3 while aged ≤12 months and CD4 count ≥500 lymphocytes/mm3 while aged 1 through 5 years.
The first dose should be administered at ages 12 months through 15 months and the second dose at ages 4 years through 6 years, or as early as 28 days after the first dose.
Individuals with perinatal HIV infection who were vaccinated prior to establishment of effective combination antiretroviral therapy (cART) should receive 2 appropriately spaced doses of MMR vaccine once effective cART has been established (for individuals aged ≤5 years: must have CD4 percentages ≥15% for ≥6 months; and for individuals aged >5 years: must have CD4 percentages ≥15% and CD4 ≥200 lymphocytes/mm3 for ≥6 months) unless they have other acceptable current evidence of measles, rubella, and mumps immunity.
Limited data are available on safety and immunogenicity of varicella vaccine in HIV-infected children aged 1 year through 8 years in CDC immunologic categories 1 and 2 (CD4 T-lymphocyte percentages 15% or greater) and clinical categories N, A, and B.
Single-antigen varicella vaccine should be considered for HIV-infected children who have CD4 percentages ≥15%. Eligible children should receive 2 doses 3 months apart, with the first dose administered as soon as possible after the first birthday.
Varicella vaccine is not recommended for HIV-infected children who have evidence of severe immunosuppression (CD4 percentage <15% at any age; for those older than age 5 years, CD4 count <200 cells/mm3).
MMRV vaccine has not been studied in HIV-infected children and should not be substituted for singleantigen varicella vaccine.
Administer to all children aged 12 months through 23 months. The 2 doses in the series should be administered at least 6 months apart.
Children who are not fully vaccinated by age 2 years can be vaccinated at subsequent visits.
HepA is also recommended for children 24 months and older who live in areas where vaccination programs target older children, who are at increased risk of infection, or for whom immunity against hepatitis A is desired. See MMWR 2006;55(No. RR-7).
Administer MCV4 to children aged 2 years through 6 years who have functional asplenia and certain other high-risk groups. A primary series of 2 doses should be administered with a minimum interval of 8 weeks. See MMWR 2007;56(48):1265–6.
Administer MCV4-D (Menactra) to infants/children 9 months through 23 months who have persistent complement component deficiency, are traveling to an area endemic for meningococcal disease, or are involved in a meningococcal outbreak.
Children who received MPSV4 ≥3 years previously and remain at increased risk of meningococcal disease should be revaccinated with MCV4.
HIV-infected children are not considered at increased risk of meningococcal disease because of HIV infection, per se. Although the efficacy of MCV4 among HIV-infected children is unknown, providers can vaccinate HIV-infected children.
HIV-infected children who remain at increased risk of meningococcal disease should be vaccinated every 5 years thereafter.
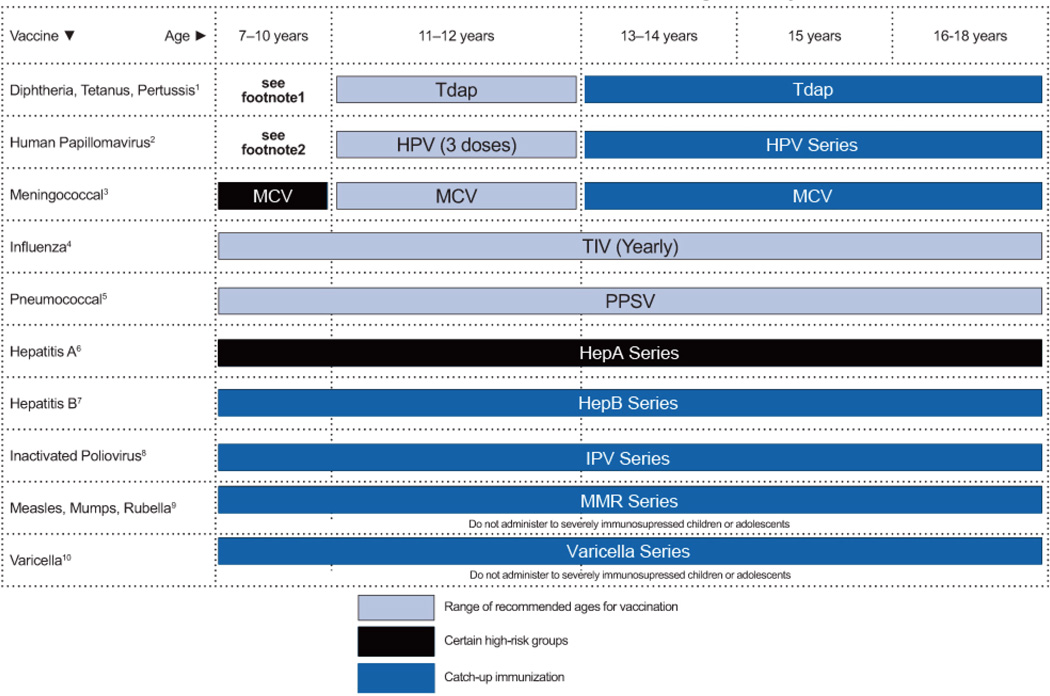
Individuals aged 11 through 18 years who have not received Tdap should receive a dose followed by Tetanus Diphtheria (Td) booster doses every 10 years thereafter.
Individuals aged 7 through 10 years who are not fully immunized against pertussis (including those never vaccinated or with unknown pertussis status) should receive a single dose of Tdap. Refer to the catch-up schedule if additional doses of tetanus and diphtheria toxoid-containing vaccine are needed.
Tdap can be administered regardless of the interval since the last tetanus dose.
HPV vaccines are most effective for both males and females when given before exposure to HPV through sexual contact.
Administer the first dose at ages 11 or 12 years.
Administer the second dose 1 to 2 months after the first dose and the third dose 6 months after the first dose (at least 24 weeks after the first dose).
Administer the series at ages 13 through 18 years if not previously vaccinated.
HPV4 can be administered in a 3-dose series to individuals aged 9 through 10 years.
Individuals who receive the second dose of the primary series at or before age 11–12 years should receive a booster dose at age 16 years. Although the efficacy of MCV4 among HIV-infected patients is unknown, HIV-infected patients aged 7 through 10 years may elect vaccination.
Administer annually to HIV-infected children and adolescents. Only TIV should be used in HIV-infected individuals. For healthy non-pregnant close contacts aged 2 through 49 years, either live, attenuated influenza vaccine (LAIV) or TIV can be used.
Administer 2 doses (separated by at least 4 weeks) to children aged younger than 9 years who are receiving influenza vaccine for the first time or based on previous influenza vaccine history, per current influenza vaccine recommendations.
A single dose of 13-valent pneumococcal conjugate vaccine (PCV13) should be routinely administered to HIV-infected children aged 6 through 18 years who did not previously receive a dose of PCV13 before age 6 years. The dose should be administered at least 8 weeks after the previous dose of PCV.
Administer 23-valent pneumococcal polysaccharide vaccine (PPSV23) at least 8 weeks after the last dose of PCV13 to children aged ≥2 years. A single revaccination dose should be administered 5 years thereafter.
HIV-infected children who have already received a dose or doses of PPSV23 should receive a dose of PCV13 a minimum of 8 weeks after the dose of PPSV23. A second dose of PPSV23 is recommended 5 years later.
HepA is recommended for children older than age 23 months who live in areas where vaccination programs target older children, who are at increased risk of infection, or for whom immunity against Hepatitis A is desired. See MMWR 2006;55(No. RR-7).
Administer the 3-dose series to those who were not previously vaccinated.
Post-vaccination testing is recommended for HIV-infected individuals. Testing should be performed 1 to 2 months after administration of the final dose. Individuals found to have anti-HBs levels of <10 mIU/mL after the primary series should be revaccinated. Administration of 3 doses on an appropriate schedule, followed by anti-HBs testing 1 to 2 months after the third dose, is usually more practical than serologic testing after 1 or 2 doses of vaccine. Modified dosing regimens, including doubling of the standard antigen dose, may increase response rates. However, data are limited on response to these alternative vaccination schedules.
In HIV-infected individuals, the need for booster doses has not been determined. Annual anti-HBs testing and booster doses when anti-HBs levels decline to <10 mIU/mL should be considered in individuals with ongoing risk of exposure. See MMWR 2005:54(No. RR-16).
The final dose in the series should be administered on or after the fourth birthday and at least 6 months after the previous dose.
For children who received an all-IPV or all-oral poliovirus (OPV) series, a fourth dose is not necessary if the third dose was administered at age ≥4 years.
If both OPV and IPV were administered as part of a series, a total of 4 doses should be administered, regardless of a child’s current age.
If eligible and not previously vaccinated, administer 2 doses with the second dose at least 28 days after the first dose, or administer the second dose for those who received only 1 dose, with at least 28 days between doses.
Two doses of MMR vaccine are recommended for all HIV-infected individuals aged ≥12 months who do not have evidence of current severe immunosuppression (i.e., individuals aged >5 years must have CD4 T lymphocyte [CD4] percentages ≥15% and CD4 ≥200 lymphocytes/mm3 for ≥6 months) or other current evidence of measles, rubella, and mumps immunity. In cases when only CD4 counts or only CD4 percentages are available for those older than age 5 years, assessment of severe immunosuppression can be based on the CD4 values (count or percentage) that are available.
Individuals with perinatal HIV infection who were vaccinated prior to establishment of effective combination antiretroviral therapy (cART) should receive two appropriately spaced doses of MMR vaccine once effective cART has been established (individuals aged >5 years: must have CD4 percentages ≥15% and CD4 ≥200 lymphocytes/mm3 for ≥6 months) unless they have other acceptable current evidence of measles, rubella, and mumps immunity.
Limited data are available on safety and immunogenicity of varicella vaccine in HIV-infected children aged 1 through 8 years in Centers for Disease Control and Prevention immunologic categories 1 and 2 (CD4 percentages ≥15%) and clinical categories N, A, and B. Varicella vaccine should be considered for HIV-infected children aged 1 through 8 years with CD4 percentages ≥15%. Eligible children should receive 2 doses at least 3 months apart.
Data are lacking on use of varicella vaccine in HIV-infected children older than age 8 years. However, on the basis of expert opinion, the safety of varicella vaccine in HIV-infected individuals older than age 8 years with similar levels of immune function (CD4 age-specific percentages ≥15% or count ≥200 cells/mm3) is likely to be similar to that for children aged ≤8 years. Immunogenicity may be lower in HIV-infected adolescents (and adults). However, weighing the risk of severe disease from wild varicella zoster virus and the potential benefit of vaccination, vaccination (2 doses administered 3 months apart) can be considered for children and adolescents aged 9 through 18 years who lack evidence of immunity.
Varicella vaccine is not recommended for HIV-infected children or adolescents who have evidence of severe immunosuppression (CD4 percentage <15% at any age; for those older than age 5 years, CD4 count <200 cells/mm3).
MMRV vaccine has not been studied in HIV-infected children and should not be substituted for single-antigen varicella vaccine.
For evidence of immunity guidance and other details, see MMWR 2007;56(No.RR-4).
Hib conjugate vaccines are available in single- or combined-antigen preparations. Hib is recommended routinely for all children through age 59 months. One dose of Hib vaccine should be administered to unvaccinated or partially vaccinated individuals aged 5 years or older who have leukemia, malignant neoplasms, anatomic or functional asplenia (including sickle cell disease), are HIV-infected, or who have other immunocompromising conditions.
References
-
- Dankner WM, Lindsey JC, Levin MJ Pediatric ACTGPT. Correlates of opportunistic infections in children infected with the human immunodeficiency virus managed before highly active antiretroviral therapy. Pediatr Infect Dis J. 2001 Jan;20(1):40–48. Available at http://www.ncbi.nlm.nih.gov/pubmed/11176565. - PubMed
-
- Gortmaker SL, Hughes M, Cervia J, et al. Effect of combination therapy including protease inhibitors on mortality among children and adolescents infected with HIV-1. N Engl J Med. 2001 Nov 22;345(21):1522–1528. Available at http://www.ncbi.nlm.nih.gov/pubmed/11794218. - PubMed
-
- Gona P, Van Dyke RB, Williams PL, et al. Incidence of opportunistic and other infections in HIV-infected children in the HAART era. JAMA. 2006 Jul 19;296(3):292–300. Available at http://www.ncbi.nlm.nih.gov/pubmed/16849662. - PubMed
-
- Nesheim SR, Kapogiannis BG, Soe MM, et al. Trends in opportunistic infections in the pre- and post-highly active antiretroviral therapy eras among HIV-infected children in the Perinatal AIDS Collaborative Transmission Study, 1986–2004. Pediatrics. 2007 Jul;120(1):100–109. Available at http://www.ncbi.nlm.nih.gov/pubmed/17606567. - PubMed
-
- Brady MT, Oleske JM, Williams PL, et al. Declines in mortality rates and changes in causes of death in HIV-1-infected children during the HAART era. J Acquir Immune Defic Syndr. 2010 Jan;53(1):86–94. Available at http://www.ncbi.nlm.nih.gov/pubmed/20035164. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
