

Long-term outcome with dasatinib after imatinib failure in chronic-phase chronic myeloid leukemia: follow-up of a phase 3 study
- PMID: 24569263
- PMCID: PMC4915794
- DOI: 10.1182/blood-2013-10-532341
Long-term outcome with dasatinib after imatinib failure in chronic-phase chronic myeloid leukemia: follow-up of a phase 3 study
Abstract
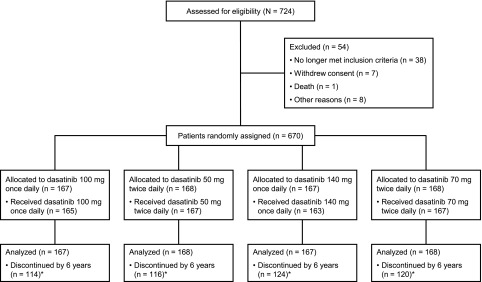
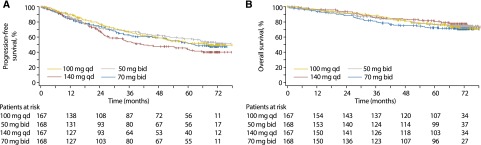
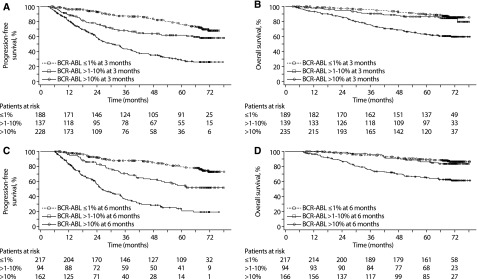
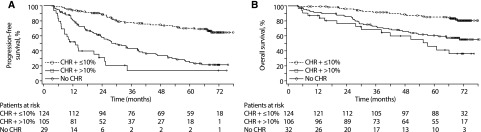
We present long-term follow-up of a dasatinib phase 3 study of patients with imatinib-resistant/-intolerant chronic myeloid leukemia (CML). In the CA180-034 study, 670 patients with imatinib-resistant/-intolerant CML in chronic phase (CML-CP) received dasatinib 100 mg once daily, 50 mg twice daily, 140 mg once daily, or 70 mg twice daily. At 6 years, 188 (28%) of 670 patients remained on study treatment. Estimated 6-year protocol-defined progression-free survival (PFS) rates were 49%, 51%, 40%, and 47%, respectively, and estimated 6-year overall survival (OS) rates were 71%, 74%, 77%, and 70%, respectively (intent-to-treat population, including protocol-defined progression or death after discontinuation). Estimated 6-year rates of survival without transformation on study treatment were 76%, 80%, 83%, and 74%, respectively. Major molecular response was achieved in 43% (100 mg once daily) and 40% (all other arms) of patients by 6 years. Molecular and cytogenetic responses at 3 and 6 months were highly predictive of PFS and OS. Notably, estimated 6-year PFS rates based on ≤1%, >1% to 10%, and >10% BCR-ABL transcripts at 3 months were 68%, 58%, and 26%, respectively. Most adverse events occurred by 2 years. Imatinib-resistant/-intolerant patients with CML-CP can experience long-term benefit with dasatinib therapy, particularly if achieving BCR-ABL ≤10% at 3 months. This study was registered at ClinicalTrials.gov: NCT00123474.
Figures
References
-
- O’Hare T, Zabriskie MS, Eiring AM, Deininger MW. Pushing the limits of targeted therapy in chronic myeloid leukaemia. Nat Rev Cancer. 2012;12(8):513–526. - PubMed
-
- Cross NCP, White HE, Müller MC, Saglio G, Hochhaus A. Standardized definitions of molecular response in chronic myeloid leukemia. Leukemia. 2012;26(10):2172–2175. - PubMed
-
- Radich JP. Monitoring response to tyrosine kinase inhibitor therapy, mutational analysis, and new treatment options in chronic myelogenous leukemia. J Natl Compr Canc Netw. 2013;11(5 suppl):663–666. - PubMed
-
- Fava C, Rege-Cambrin G, Saglio G. Chronic myeloid leukemia: state of the art in 2012. Curr Oncol Rep. 2012;14(5):379–386. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
