

Coagulopathy after severe pediatric trauma
- PMID: 24569507
- PMCID: PMC4024323
- DOI: 10.1097/SHK.0000000000000151
Coagulopathy after severe pediatric trauma
Abstract
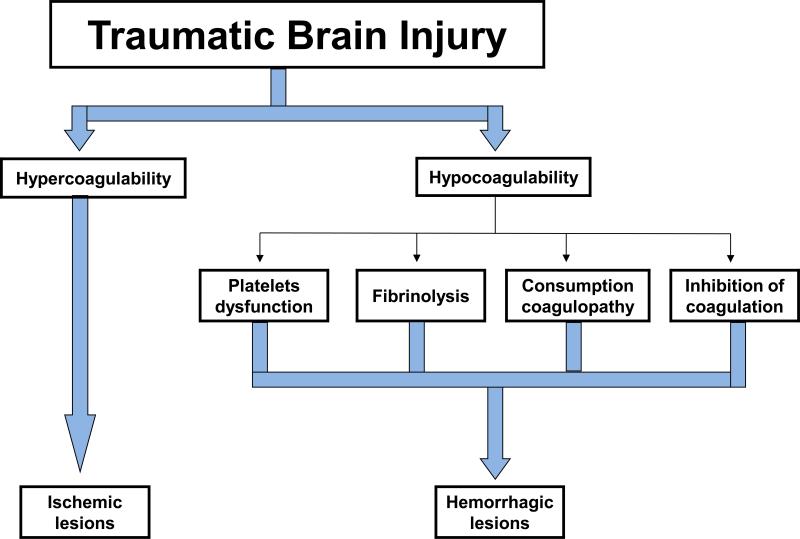
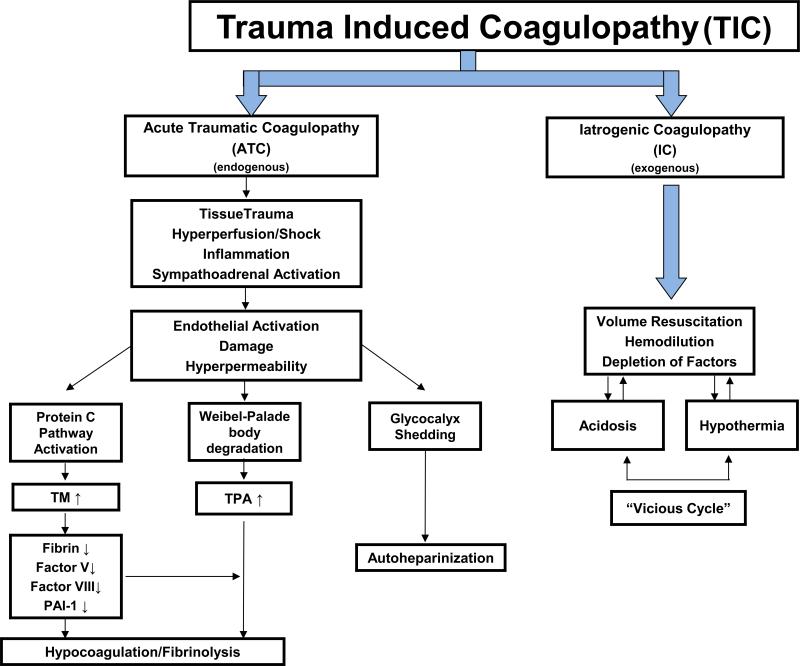
Trauma remains the leading cause of morbidity and mortality in the United States among children aged 1 to 21 years. The most common cause of lethality in pediatric trauma is traumatic brain injury. Early coagulopathy has been commonly observed after severe trauma and is usually associated with severe hemorrhage and/or traumatic brain injury. In contrast to adult patients, massive bleeding is less common after pediatric trauma. The classical drivers of trauma-induced coagulopathy include hypothermia, acidosis, hemodilution, and consumption of coagulation factors secondary to local activation of the coagulation system after severe traumatic injury. Furthermore, there is also recent evidence for a distinct mechanism of trauma-induced coagulopathy that involves the activation of the anticoagulant protein C pathway. Whether this new mechanism of posttraumatic coagulopathy plays a role in children is still unknown. The goal of this review is to summarize the current knowledge on the incidence and potential mechanisms of coagulopathy after pediatric trauma and the role of rapid diagnostic tests for early identification of coagulopathy. Finally, we discuss different options for treating coagulopathy after severe pediatric trauma.
Figures
References
-
- Avarello JT, Cantor RM. Pediatric major trauma: an approach to evaluation and management. Emerg Med Clin North Am. 2007;25(3):803–836. - PubMed
-
- Mace SE, Gerardi MJ, Dietrich AM, Knazik SR, Mulligan-Smith D, Sweeney RL, Warden CR. Injury prevention and control in children. Ann Emerg Med. 2001;38(4):405–414. - PubMed
-
- Brohi K, Singh J, Heron M, Coats T. Acute traumatic coagulopathy. The Journal of trauma. 2003;54(6):1127–1130. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
