

Reduced nocturnal ACTH-driven cortisol secretion during critical illness
- PMID: 24569590
- PMCID: PMC3989736
- DOI: 10.1152/ajpendo.00009.2014
Reduced nocturnal ACTH-driven cortisol secretion during critical illness
Abstract
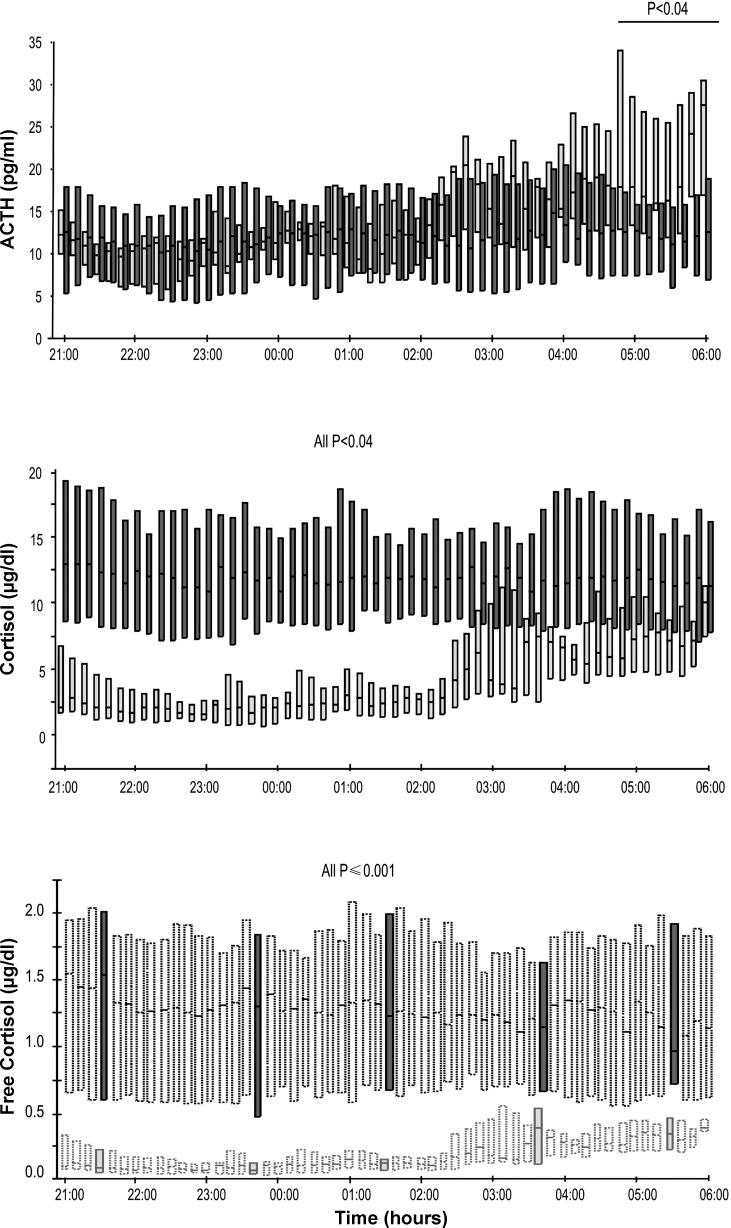
Recently, during critical illness, cortisol metabolism was found to be reduced. We hypothesize that such reduced cortisol breakdown may suppress pulsatile ACTH and cortisol secretion via feedback inhibition. To test this hypothesis, nocturnal ACTH and cortisol secretory profiles were constructed by deconvolution analysis from plasma concentration time series in 40 matched critically ill patients and eight healthy controls, excluding diseases or drugs that affect the hypothalamic-pituitary-adrenal axis. Blood was sampled every 10 min between 2100 and 0600 to quantify plasma concentrations of ACTH and (free) cortisol. Approximate entropy, an estimation of process irregularity, cross-approximate entropy, a measure of ACTH-cortisol asynchrony, and ACTH-cortisol dose-response relationships were calculated. Total and free plasma cortisol concentrations were higher at all times in patients than in controls (all P < 0.04). Pulsatile cortisol secretion was 54% lower in patients than in controls (P = 0.005), explained by reduced cortisol burst mass (P = 0.03), whereas cortisol pulse frequency (P = 0.35) and nonpulsatile cortisol secretion (P = 0.80) were unaltered. Pulsatile ACTH secretion was 31% lower in patients than in controls (P = 0.03), again explained by a lower ACTH burst mass (P = 0.02), whereas ACTH pulse frequency (P = 0.50) and nonpulsatile ACTH secretion (P = 0.80) were unchanged. ACTH-cortisol dose response estimates were similar in patients and controls. ACTH and cortisol approximate entropy were higher in patients (P ≤ 0.03), as was ACTH-cortisol cross-approximate entropy (P ≤ 0.001). We conclude that hypercortisolism during critical illness coincided with suppressed pulsatile ACTH and cortisol secretion and a normal ACTH-cortisol dose response. Increased irregularity and asynchrony of the ACTH and cortisol time series supported non-ACTH-dependent mechanisms driving hypercortisolism during critical illness.
Keywords: adrenocorticotropic hormone; cortisol; deconvolution analysis; intensive care; secretion.
Figures



References
-
- Annane D, Sebille V, Charpentier C, Bollaert PE, Francois B, Korach JM, Capellier G, Cohen Y, Azoulay E, Troche G, Chaumet-Riffaud P, Bellissant E. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA 288: 862–871, 2002 - PubMed
-
- Bornstein SR. Predisposing factors for adrenal insufficiency. N Engl J Med 360: 2328–2339, 2009 - PubMed
-
- Bornstein SR, Chrousos GP. Clinical review 104: Adrenocorticotropin (ACTH)- and non-ACTH-mediated regulation of the adrenal cortex: neural and immune inputs. J Clin Endocrinol Metab 84: 1729–1736, 1999 - PubMed
-
- Bornstein SR, Engeland WC, Ehrhart-Bornstein M, Herman JP. Dissociation of ACTH and glucocorticoids. Trends Endocrinol Metab 19: 175–180, 2008 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources