

Accuracy of bony landmarks for restoring the natural joint line in revision knee surgery: an MRI study
- PMID: 24570152
- PMCID: PMC4037526
- DOI: 10.1007/s00264-014-2292-3
Accuracy of bony landmarks for restoring the natural joint line in revision knee surgery: an MRI study
Abstract
Purpose: Restoring the joint line (JL) improves clinical and functional outcome in total knee arthroplasty (TKA). Therefore, anatomical landmarks to approximate the JL have been published. So far, the natural deviation of the JL 90° to the mechanical tibial axis has not been considered. Thus, we designed this study to: (1) determine the natural JL of knees in healthy persons in respect to the mechanical tibial axis, (2) validate and double-check intra-operative bony landmarks already been published in respect to the natural JL and (3) find possible correlations between distances from bony landmarks to the JL and femoral and tibial width.
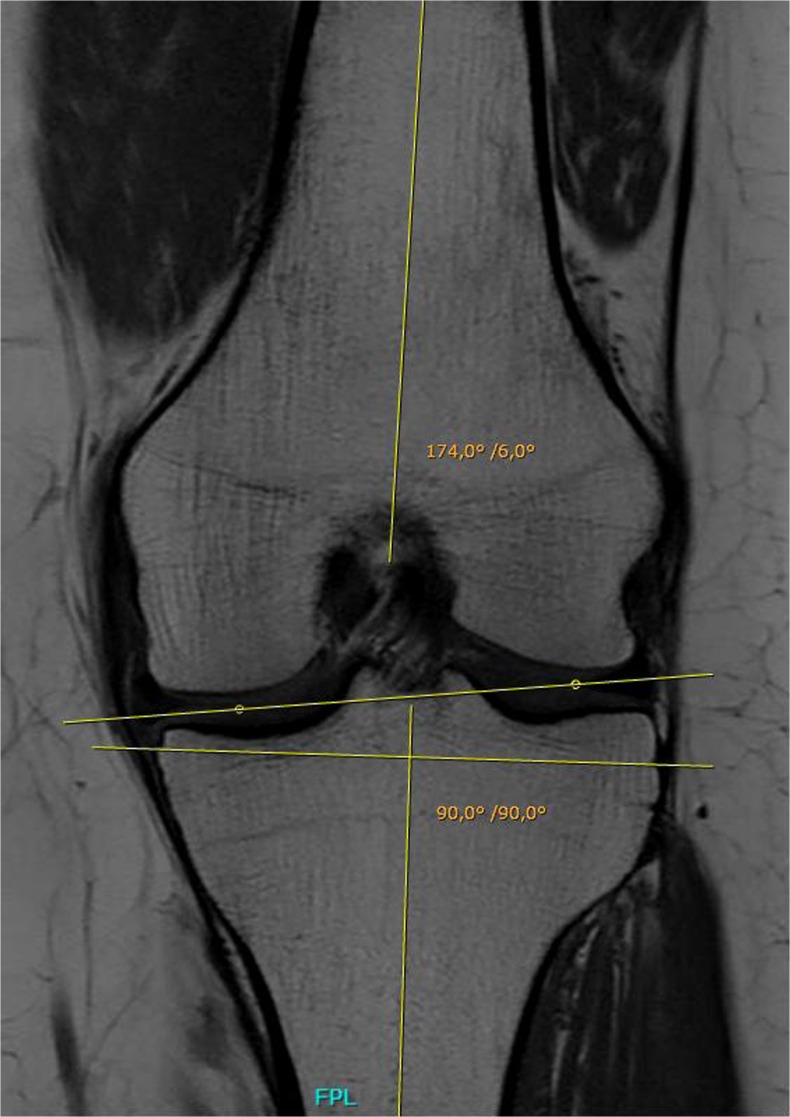
Methods: Eighty MRI scans of knees of healthy persons were examined by two independent observers. Distances from the tip of the fibular head (FH), the medial (ME) and lateral (LE) epicondyles and the adductor tubercle (AT) to the JL within the medial and lateral compartment were measured. Further, we determined the orientation of the JL in respect to the mechanical axis of the tibia. Interobserver correlations were calculated. Differences were analyzed using Student's t test. Linear regression models were calculated to analyze correlations.
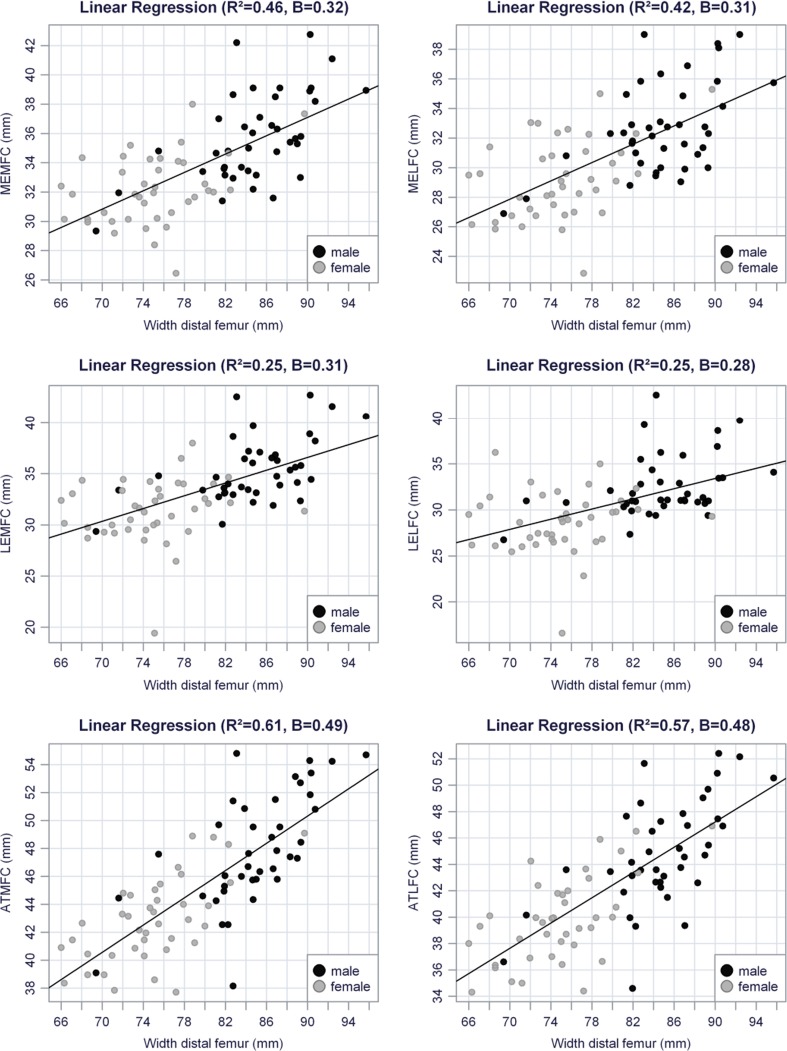
Results: Interobserver correlation was excellent. Mean JL deviation was 4.2° varus. Distance between the FH, ME, LE and AT to the JL within the medial compartment was 12.2, 33.9, 33.4 and 45.4 mm, respectively. Within in the lateral compartment, distances were 15.3, 31.0, 30.6 and 42.3 mm to the JL. Strong correlation was found between femoral width and distances from the AT, ME and LE to the JL.
Conclusion: In TKA, the JL is usually altered due to the classic resection technique, which does not respect the natural deviation of the JL. Estimating the natural JL by adding absolute values to bony landmarks, as proposed in the literature, is not recommended. According to our data, the JL can be best estimated by adding the calculated value: 6.40 + (width femur [mm] × 0.49) to the AT.
Figures


References
-
- Martin JW, Whiteside LA. The influence of joint line position on knee stability after condylar knee arthroplasty. Clin Orthop. 1990;259:146. - PubMed
-
- Figgie HE, III, Goldberg VM, Heiple KG, Moller HS, III, Gordon NH. The influence of tibial-patellofemoral location on function of the knee in patients with the posterior stabilized condylar knee prosthesis. J Bone Joint Surg Am. 1986;68:1035–1040. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
