

Urinary tract infections in older women: a clinical review
- PMID: 24570248
- PMCID: PMC4194886
- DOI: 10.1001/jama.2014.303
Urinary tract infections in older women: a clinical review
Abstract
Importance: Asymptomatic bacteriuria and symptomatic urinary tract infections (UTIs) in older women are commonly encountered in outpatient practice.
Objective: To review management of asymptomatic bacteriuria and symptomatic UTI and review prevention of recurrent UTIs in older community-dwelling women.
Evidence review: A search of Ovid (Medline, PsycINFO, Embase) for English-language human studies conducted among adults aged 65 years and older and published in peer-reviewed journals from 1946 to November 20, 2013.
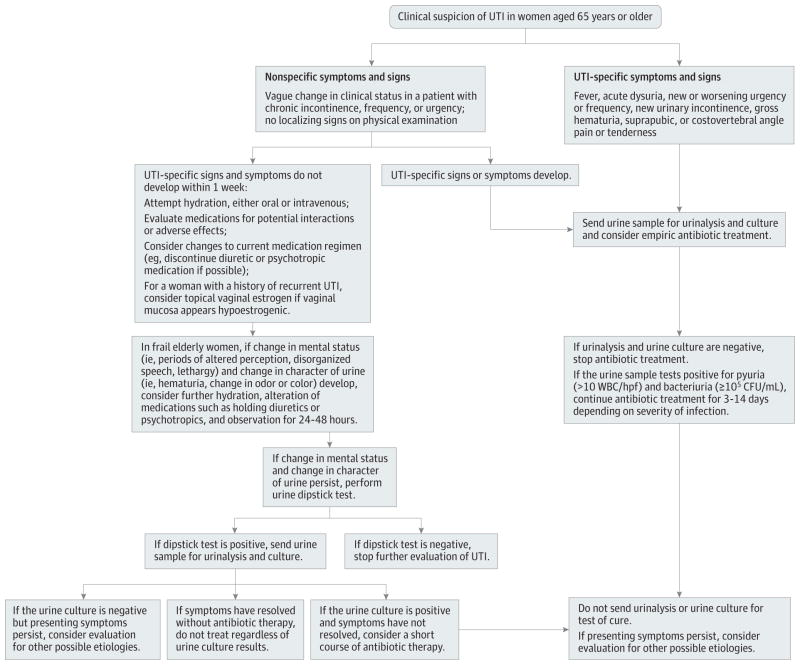
Results: The clinical spectrum of UTIs ranges from asymptomatic bacteriuria, to symptomatic and recurrent UTIs, to sepsis associated with UTI requiring hospitalization. Recent evidence helps differentiate asymptomatic bacteriuria from symptomatic UTI. Asymptomatic bacteriuria is transient in older women, often resolves without any treatment, and is not associated with morbidity or mortality. The diagnosis of symptomatic UTI is made when a patient has both clinical features and laboratory evidence of a urinary infection. Absent other causes, patients presenting with any 2 of the following meet the clinical diagnostic criteria for symptomatic UTI: fever, worsened urinary urgency or frequency, acute dysuria, suprapubic tenderness, or costovertebral angle pain or tenderness. A positive urine culture (≥105 CFU/mL) with no more than 2 uropathogens and pyuria confirms the diagnosis of UTI. Risk factors for recurrent symptomatic UTI include diabetes, functional disability, recent sexual intercourse, prior history of urogynecologic surgery, urinary retention, and urinary incontinence. Testing for UTI is easily performed in the clinic using dipstick tests. When there is a low pretest probability of UTI, a negative dipstick result for leukocyte esterase and nitrites excludes infection. Antibiotics are selected by identifying the uropathogen, knowing local resistance rates, and considering adverse effect profiles. Chronic suppressive antibiotics for 6 to 12 months and vaginal estrogen therapy effectively reduce symptomatic UTI episodes and should be considered in patients with recurrent UTIs.
Conclusions and relevance: Establishing a diagnosis of symptomatic UTI in older women requires careful clinical evaluation with possible laboratory assessment using urinalysis and urine culture. Asymptomatic bacteriuria should be differentiated from symptomatic UTI. Asymptomatic bacteriuria in older women should not be treated.
Conflict of interest statement
Figures
References
-
- Foxman B. Epidemiology of urinary tract infections. Dis Mon. 2003;49(2):53–70. - PubMed
-
- Litwin MS, Saigal CS, Yano EM, et al. Urologic Diseases in America Project. Urologic diseases in america Project. J Urol. 2005;173(3):933–937. - PubMed
-
- Sobel JD, Kaye D. Urinary tract infections. In: Mandell Gl, Bennett JC, Dolin R., editors. Mandell, Douglas, and Bennett’s: Principles and Practice of Infectious Disease. 7. Philadelphia, PA: Elsevier; 2010. p. 957.
-
- Monane M, Gurwitz JH, Lipsitz LA, Glynn RJ, Choodnovskiy I, Avorn J. Epidemiologic and diagnostic aspects of bacteriuria: a longitudinal study in older women. J Am Geriatr Soc. 1995;43(6):618–622. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
