

Correlation between 3D-MRCP and intra-operative findings in right liver donors
- PMID: 24570909
- PMCID: PMC3924642
- DOI: 10.3978/j.issn.2304-3881.2012.11.01
Correlation between 3D-MRCP and intra-operative findings in right liver donors
Abstract
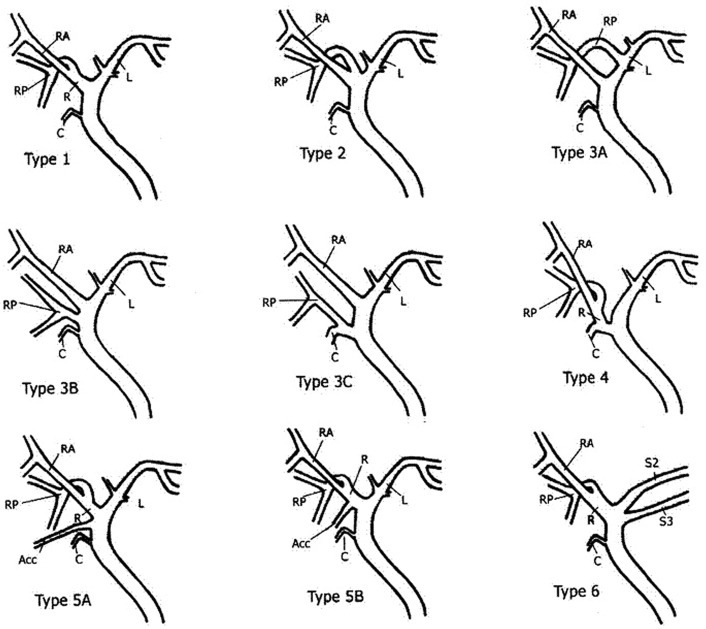
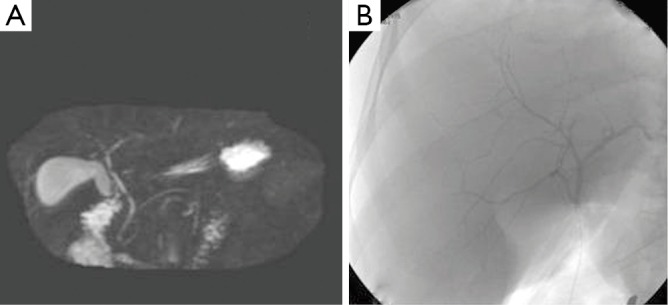
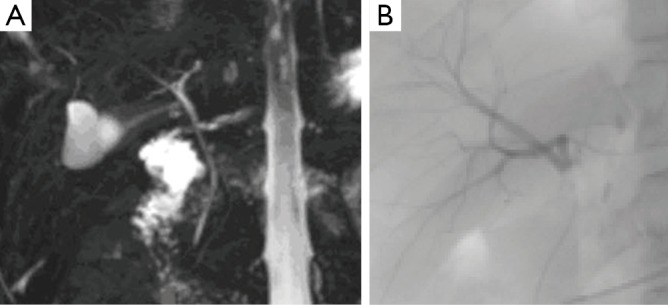
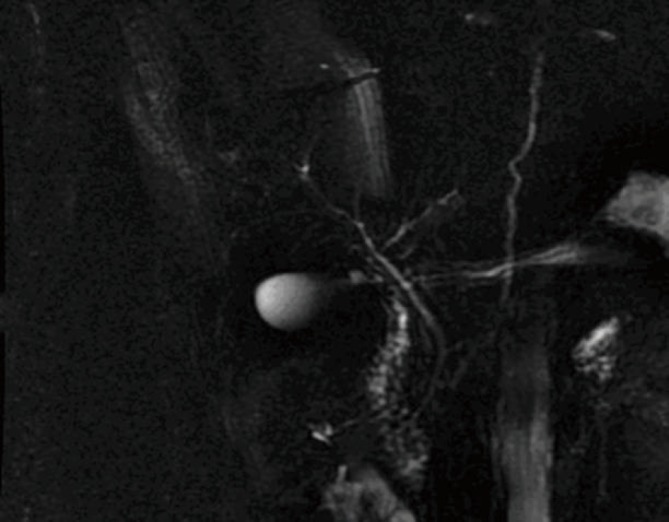
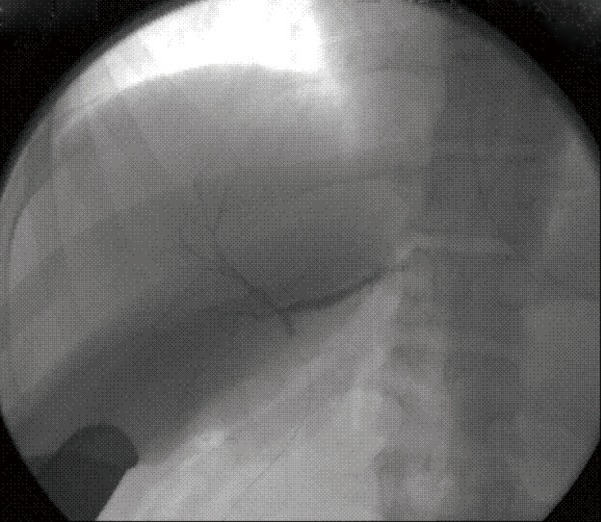
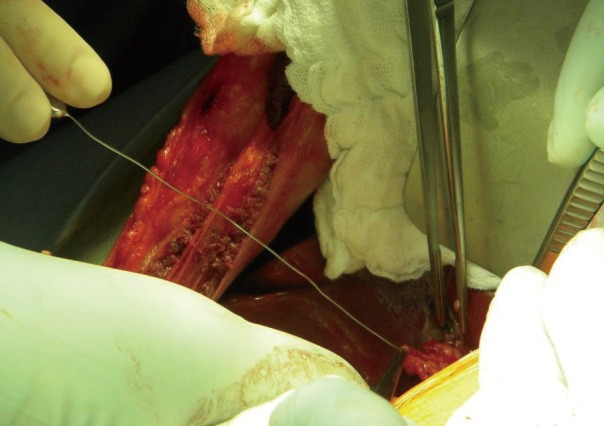
A correct preoperative definition of the hepatic duct confluence anatomy of right liver living donors is a pivotal step in determining their candidacy for donation and planning the surgery. The purposes of this study are to evaluate the accuracy of three-dimensional Magnetic Resonance Cholangiography (3D MRCP) when compared with intraoperative cholangiography (IOC) in assessing biliary anatomy and to identify imaging characteristics that may help predict the yield of hepatic duct orifices in the right liver graft. Twenty consecutive right liver donors were imaged with 3D MRCP and IOC. The MRCP and IOC findings were compared, and the results confirmed against actual donor anatomy. Three-D MRCP accurately predicted the biliary anatomy in 18 of 20 cases. Specificity and positive predictive value of 3D MRCP in defining normal biliary anatomy was 100%. In 2 patients, 3D MRCP failed to indentify abnormal anatomy. The yield of more than one hepatic duct was associated with: (I) The presence of abnormal biliary anatomy, (II) The length of the main right hepatic duct, and (III) The presence of an acute angle at the confluence of right and left hepatic duct. In conclusion, 3D MRCP reliably represents normal biliary anatomy. The presence of anatomical variations decreases MRCP sensitivity and makes IOC or duct probing a necessary tool for accurately performing the transection of the right hepatic duct.
Keywords: Cholangiogram; live donors; liver transplantation; magnetic resonance cholangio-pancreaticogram (MRCP); preoperative evaluation.
Figures
References
-
- Kashyap R, Bozorgzadeh A, Abt P, et al. Stratifying risk of biliary complications in adult living donor liver transplantation by magnetic resonance cholangiography. Transplantation 2008;85:1569-72 - PubMed
-
- Nakamura T, Tanaka K, Kiuchi T, et al. Anatomical variations and surgical strategies in right lobe living donor liver transplantation: lessons from 120 cases. Transplantation 2002;73:1896-903 - PubMed
-
- Hwang S, Lee SG, Sung KB, et al. Long-term incidence, risk factors, and management of biliary complications after adult living donor liver transplantation. Liver Transpl 2006;12:831-8 - PubMed
-
- Yeh BM, Breiman RS, Taouli B, et al. Biliary tract depiction in living potential liver donors: comparison of conventional MR, mangafodipir trisodium-enhanced excretory MR, and multi-detector row CT cholangiography--initial experience. Radiology 2004;230:645-51 - PubMed
LinkOut - more resources
Full Text Sources