

Economic evaluation of a hypothetical screening assay for alloimmunization risk among transfused patients with sickle cell disease
- PMID: 24571485
- PMCID: PMC4138280
- DOI: 10.1111/trf.12585
Economic evaluation of a hypothetical screening assay for alloimmunization risk among transfused patients with sickle cell disease
Abstract
Background: Prophylactic antigen-matching can reduce alloimmunization rates among chronically transfused patients with sickle cell disease (SCD), but this matching increases costs and may only benefit 30% of patients. We assessed the clinical and financial value of a potential assay for alloimmunization risk that would allow for targeted antigen-matching.
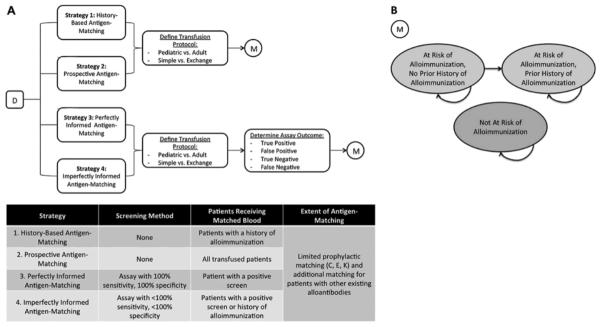
Study design and methods: A Markov-based model evaluated direct medical costs and alloimmunization events over 10 to 20 years among transfused (simple or exchange) patients with SCD. Four matching strategies were evaluated: prospective matching (for all patients), history-based matching (only for patients with prior alloimmunization), perfectly informed matching (assay with 100% sensitivity, 100% specificity), and imperfectly informed matching (reduced accuracy). Under all matching protocols, matching included C, E, K, and any additional alloantibodies present. A hospital perspective was adopted, with costs (2012US$) and events discounted (3%).
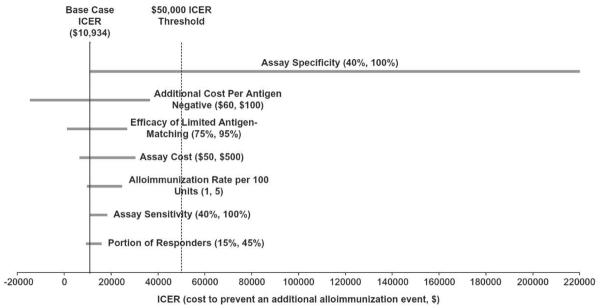
Results: Perfectly informed antigen-matching using a $1000 assay is expected to save $82,334 per patient over 10 years, compared to prospective matching. Perfectly informed antigen-matching is more costly than history-based matching, but reduces alloimmunization events by 45.6% over 10 years. Averting each alloimmunization event using this strategy would cost an additional $10,934 per patient. Imperfectly informed antigen-matching using an assay with 75% specificity and 75% sensitivity is less costly than prospective matching, but increases alloimmunization events. Compared to history-based matching, imperfectly informed matching would decrease alloimmunization events by 32.61%, at an additional cost of $147,915 per patient over 10 years. Cost-effectiveness of informed antigen-matching is largely driven by assay specificity.
Conclusions: A sufficiently specific assay to inform antigen-matching may be cost-effective in reducing alloimmunization among transfused patients with SCD.
© 2014 AABB.
Figures
References
-
- Vichinsky EP, Earles A, Johnson RA, Hoag MS, Williams A, Lubin B. Alloimmunization in sickle cell anemia and transfusion of racially unmatched blood. N Engl J Med. 1990;322:1617–21. - PubMed
-
- Rosse WF, Gallagher D, Kinney TR, Castro O, Dosik H, Moohr J, Wang W, Levy PS. Transfusion and alloimmunization in sickle cell disease. The Cooperative Study of Sickle Cell Disease. Blood. 1990;76:1431–7. - PubMed
-
- Lasalle-Williams M, Nuss R, Le T, Cole L, Hassell K, Murphy JR, Ambruso DR. Extended red blood cell antigen matching for transfusions in sickle cell disease: a review of a 14-year experience from a single center (CME) Transfusion. 2011;51:1732–9. - PubMed
-
- Vichinsky EP. The prevention and management of alloimmunization in sickle cell disease: the benefit of extended phenotypic matching of red blood cells. Immunohematology. 2012;28:20–3. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
