

Reliability of CT perfusion in the evaluation of the ischaemic penumbra
- PMID: 24571838
- PMCID: PMC4202849
- DOI: 10.15274/NRJ-2014-10010
Reliability of CT perfusion in the evaluation of the ischaemic penumbra
Abstract
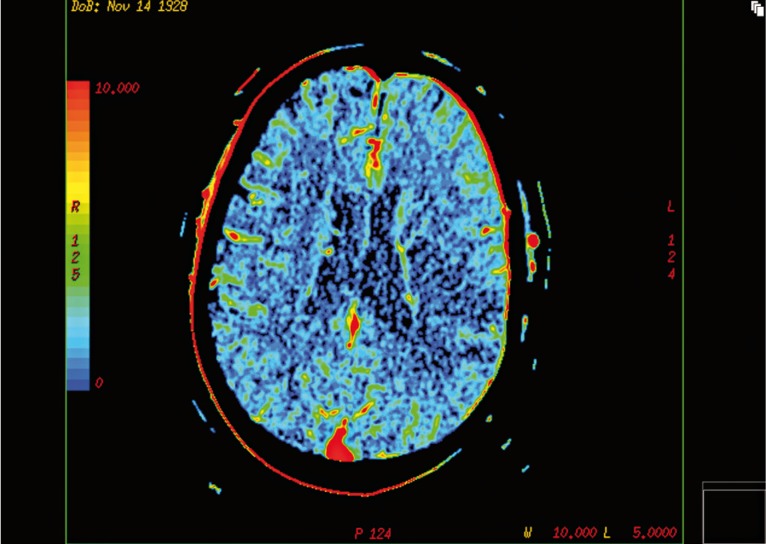
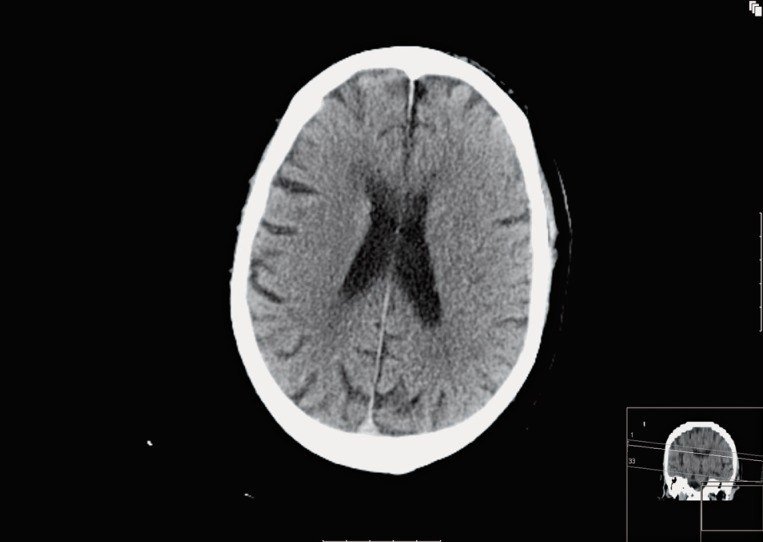
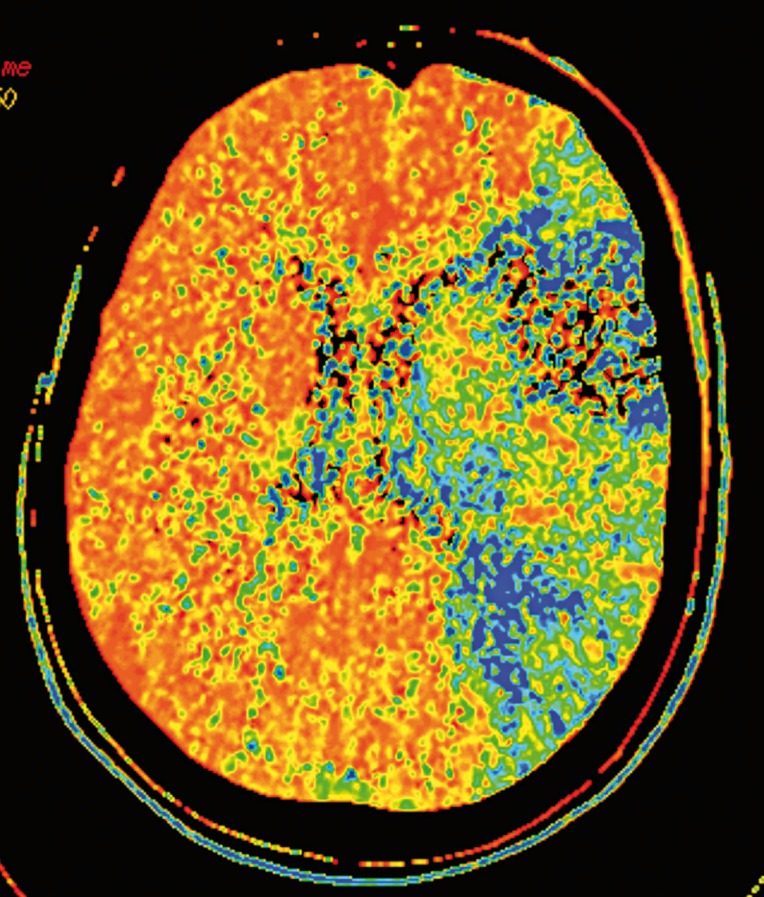
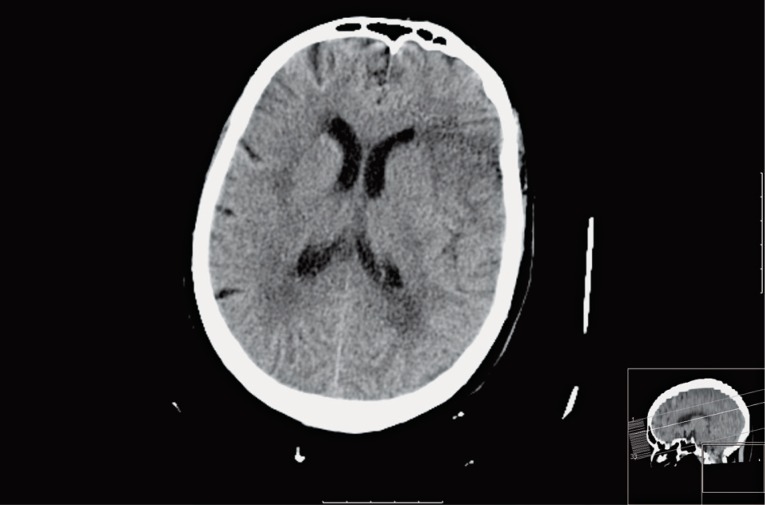
CT perfusion (CTP) is part of the initial evaluation of stroke patients, allowing differentiation between infarcted tissue and the ischaemic penumbra and helping in the selection of patients for endovascular treatment. This study assessed the reliability of the qualitative evaluation CTP maps in defining the ischemic penumbra and identified potential pitfalls associated with this technique. We reviewed CTP scans of 45 consecutive patients admitted to our institution with anterior circulation acute ischaemic stroke. Two neuroradiologists performed qualitative evaluations of cerebral blood volume (CBV) and mean transit time (MTT) maps, using 24h follow-up non-contrast CT as surrogate marker for the area of definitive infarct. For each slice analyzed, the area of qualitative alteration in the CBV and MTT maps was classified as either being inferior, equal or superior to the area of infarct on the follow-up CT. Three out of 45 (7%) patients had admission CT CBV abnormalities larger than follow-up lesions; 34/45 (76%) patients had infarct areas smaller than initial MTT prolongation. In the group of patients with no recanalization 12/19 (63%) had infarct areas smaller than initial MTT lesion. CBV abnormality is a reliable marker for an irreversible ischaemic lesion, although rarely it may overestimate the ischaemic "core", possibly due to delay in contrast arrival to the brain. In the majority of patients without recanalization, MTT overestimated final infarct areas, probably because it does not differentiate true "at risk" penumbra from benign oligaemia. Qualitative evaluation of CBV and MTT maps may overestimate the real ischaemic penumbra.
Keywords: CT perfusion; acute stroke; brain infarction; cerebral blood volume; endovascular treatment.
Figures
Comment in
-
Letter to the Editor. CT angiography source-images and CT perfusion: are they complementary tools for ischemic stroke evaluation? Response to: reliability of CT perfusion in the evaluation of ischaemic penumbra.Neuroradiol J. 2014 Jun;27(3):365-7. doi: 10.15274/NRJ-2014-10043. Epub 2014 Jun 17. Neuroradiol J. 2014. PMID: 24976206 Free PMC article. No abstract available.
-
Response to letter to the editor. "CT angiography source-images and CT perfusion: are they complementary tools for ischemic stroke evaluation?".Neuroradiol J. 2014 Jun;27(3):368. doi: 10.15274/NRJ-2014-10044. Epub 2014 Jun 17. Neuroradiol J. 2014. PMID: 24976207 Free PMC article. No abstract available.
Similar articles
-
Clinical use of computed tomographic perfusion for the diagnosis and prediction of lesion growth in acute ischemic stroke.J Stroke Cerebrovasc Dis. 2014 Jan;23(1):114-22. doi: 10.1016/j.jstrokecerebrovasdis.2012.10.020. Epub 2012 Dec 14. J Stroke Cerebrovasc Dis. 2014. PMID: 23253533 Free PMC article.
-
Incorporation of relative cerebral blood flow into CT perfusion maps reduces false 'at risk' penumbra.J Neurointerv Surg. 2018 Jul;10(7):657-662. doi: 10.1136/neurintsurg-2017-013268. Epub 2017 Sep 30. J Neurointerv Surg. 2018. PMID: 28965105
-
Perfusion CT in acute stroke: predictive value of perfusion parameters in assessing tissue viability versus infarction.Radiol Med. 2007 Feb;112(1):113-22. doi: 10.1007/s11547-007-0125-9. Epub 2007 Feb 22. Radiol Med. 2007. PMID: 17310286 English, Italian.
-
Theoretic basis and technical implementations of CT perfusion in acute ischemic stroke, part 1: Theoretic basis.AJNR Am J Neuroradiol. 2009 Apr;30(4):662-8. doi: 10.3174/ajnr.A1487. Epub 2009 Mar 6. AJNR Am J Neuroradiol. 2009. PMID: 19270105 Free PMC article. Review.
-
Imaging viable brain tissue with CT scan during acute stroke.Cerebrovasc Dis. 2004;17 Suppl 3:28-34. doi: 10.1159/000075302. Cerebrovasc Dis. 2004. PMID: 14730256 Review.
Cited by
-
Perfluorocarbon Enhanced Glasgow Oxygen Level Dependent (GOLD) Magnetic Resonance Metabolic Imaging Identifies the Penumbra Following Acute Ischemic Stroke.Theranostics. 2018 Feb 12;8(6):1706-1722. doi: 10.7150/thno.21685. eCollection 2018. Theranostics. 2018. PMID: 29556351 Free PMC article.
-
Imaging evaluation of acute ischemic stroke.J Int Med Res. 2020 Jan;48(1):300060518802530. doi: 10.1177/0300060518802530. J Int Med Res. 2020. PMID: 31997680 Free PMC article. No abstract available.
-
Cerebral vasospasm and hypoperfusion after traumatic brain injury: Combined CT angiography and CT perfusion imaging study.Surg Neurol Int. 2021 Jul 19;12:361. doi: 10.25259/SNI_859_2020. eCollection 2021. Surg Neurol Int. 2021. PMID: 34345501 Free PMC article.
-
Current concepts on magnetic resonance imaging (MRI) perfusion-diffusion assessment in acute ischaemic stroke: a review & an update for the clinicians.Indian J Med Res. 2014 Dec;140(6):717-28. Indian J Med Res. 2014. PMID: 25758570 Free PMC article. Review.
-
Comparative accuracy of CT perfusion in diagnosing acute ischemic stroke: A systematic review of 27 trials.PLoS One. 2017 May 17;12(5):e0176622. doi: 10.1371/journal.pone.0176622. eCollection 2017. PLoS One. 2017. PMID: 28520753 Free PMC article.
References
-
- Baron JC. Mapping the ischaemic penumbra with PET: implications for acute stroke treatment. Cerebrovasc Dis. 1999;9(4):93–201. doi: 10.1159/000015955. - DOI - PubMed
-
- Alawneh JA, Jones PS, Mikkelsen IK, et al. Infarction of ‘non-core-non-penumbral’ tissue after stroke: multivariate modelling of clinical impact. Brain. 2011;134(Pt 6):1765–1776. doi: 10.1093/brain/awr100. - DOI - PubMed
-
- Yoo AJ, Chaudhry ZA, Nogueira RG, et al. Infarct volume is a pivotal biomarker after intra-arterial stroke therapy. Stroke. 2012;43(5):1323–1330. doi: 10.1161/STROKEAHA.111.639401. - DOI - PubMed
-
- Zaidi SF, Aghaebrahim A, Urra X, et al. Final infarct volume is a stronger predictor of outcome than recanalization in patients with proximal middle cerebral artery occlusion treated with endovascular therapy. Stroke. 2012;43(12):3238–3244. doi: 10.1161/STROKEAHA.112.671594. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
