

Tactile acuity training for patients with chronic low back pain: a pilot randomised controlled trial
- PMID: 24571855
- PMCID: PMC3942257
- DOI: 10.1186/1471-2474-15-59
Tactile acuity training for patients with chronic low back pain: a pilot randomised controlled trial
Abstract
Background: Chronic pain can disrupt the cortical representation of a painful body part. This disruption may play a role in maintaining the individual's pain. Tactile acuity training has been used to normalise cortical representation and reduce pain in certain pain conditions. However, there is little evidence for the effectiveness of this intervention for chronic low back pain (CLBP). The primary aim of this study was to inform the development of a fully powered randomised controlled trial (RCT) by providing preliminary data on the effect of tactile acuity training on pain and function in individuals with CLBP. The secondary aim was to obtain qualitative feedback about the intervention.
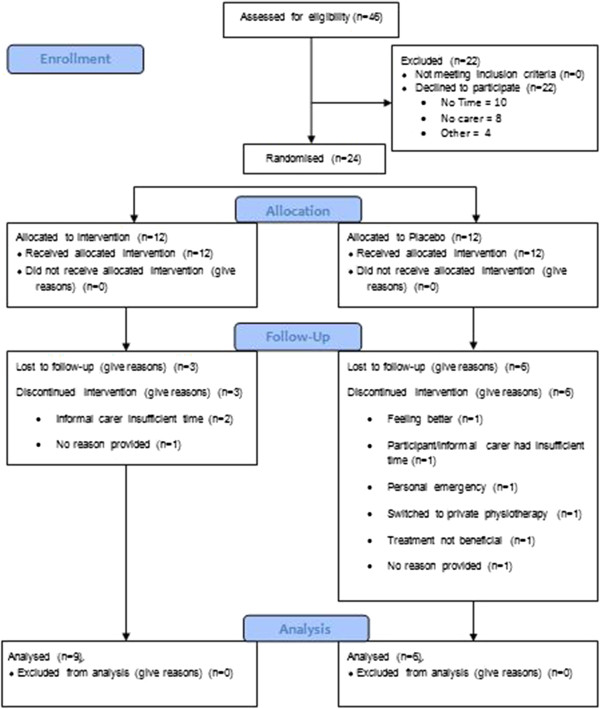
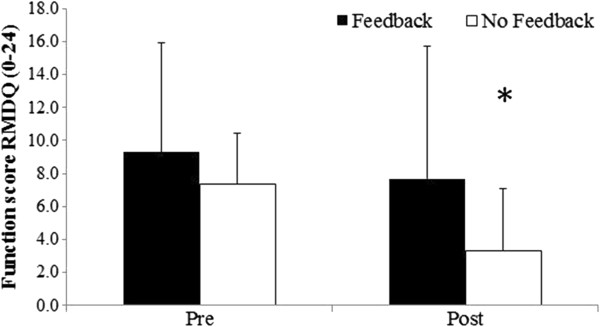
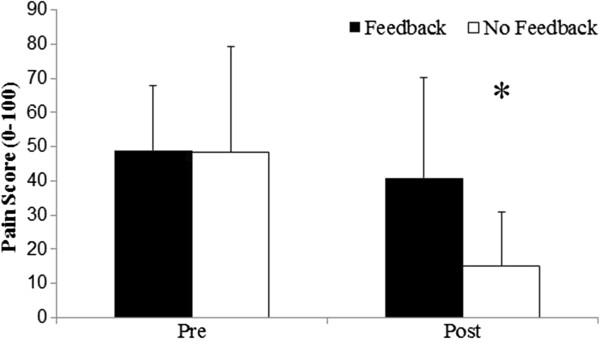
Methods: In this mixed-methods pilot RCT 15 individuals were randomised to either an intervention (tactile acuity training) or a placebo group (sham tactile acuity training). All participants received 3 sessions of acuity training (intervention or sham) from a physiotherapist and were requested to undertake daily acuity home training facilitated by an informal carer (friend/relative). All participants also received usual care physiotherapy. The primary outcome measures were pain (0-100visual analogue scale (VAS)) and function (Roland Morris Disability Questionnaire (RMDQ)). Participants and their informal carers were invited to a focus group to provide feedback on the intervention.
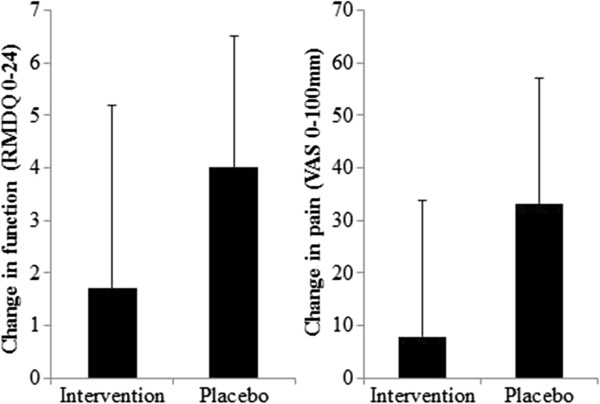
Results: The placebo group improved by the greatest magnitude for both outcome measures, but there was no statistically significant difference (Mean difference (95%CI), p-value) between groups for change in pain (25.6 (-0.7 to 51.9), p = 0.056) or function (2.2 (-1.6 to 6.0), p = 0.237). Comparing the number of individuals achieving a minimally clinically significant improvement, the placebo group had better outcomes for pain with all participants achieving ≥30% improvement compared to only a third of the intervention group (6/6 vs. 3/9, p = 0.036). Qualitatively, participants reported that needing an informal carer was a considerable barrier to the home training component of the study.
Conclusions: This pilot RCT found tactile acuity training to be no more effective than sham tactile acuity training for function and less effective for pain in individuals with CLBP. That the intervention could not be self-applied was a considerable barrier to its use.
Trial registration isrctn: ISRCTN98118082.
Figures
Similar articles
-
Reduced tactile acuity in chronic low back pain is linked with structural neuroplasticity in primary somatosensory cortex and is modulated by acupuncture therapy.Neuroimage. 2020 Aug 15;217:116899. doi: 10.1016/j.neuroimage.2020.116899. Epub 2020 May 5. Neuroimage. 2020. PMID: 32380138 Free PMC article. Clinical Trial.
-
The effect of changing movement and posture using motion-sensor biofeedback, versus guidelines-based care, on the clinical outcomes of people with sub-acute or chronic low back pain-a multicentre, cluster-randomised, placebo-controlled, pilot trial.BMC Musculoskelet Disord. 2015 May 29;16:131. doi: 10.1186/s12891-015-0591-5. BMC Musculoskelet Disord. 2015. PMID: 26022102 Free PMC article. Clinical Trial.
-
Short-term effect on pain and function of neurophysiological education and sensorimotor retraining compared to usual physiotherapy in patients with chronic or recurrent non-specific low back pain, a pilot randomized controlled trial.BMC Musculoskelet Disord. 2015 Apr 10;16:83. doi: 10.1186/s12891-015-0533-2. BMC Musculoskelet Disord. 2015. PMID: 25887550 Free PMC article. Clinical Trial.
-
In trials of physiotherapy for chronic low back pain, clinical relevance is rarely interpreted, with great heterogeneity in the frameworks and thresholds used: a meta-research study.J Physiother. 2024 Jan;70(1):51-64. doi: 10.1016/j.jphys.2023.11.007. Epub 2023 Dec 9. J Physiother. 2024. PMID: 38072712 Review.
-
Associative fear learning and perceptual discrimination: a perceptual pathway in the development of chronic pain.Neurosci Biobehav Rev. 2015 Apr;51:118-25. doi: 10.1016/j.neubiorev.2015.01.009. Epub 2015 Jan 17. Neurosci Biobehav Rev. 2015. PMID: 25603316 Review.
Cited by
-
Manual Therapy versus Localisation (Tactile, Sensory Training) in Patients with Non-Specific Neck Pain: A Randomised Clinical Pilot Trial.Healthcare (Basel). 2023 May 11;11(10):1385. doi: 10.3390/healthcare11101385. Healthcare (Basel). 2023. PMID: 37239671 Free PMC article.
-
The translation, validity and reliability of the German version of the Fremantle Back Awareness Questionnaire.PLoS One. 2018 Oct 4;13(10):e0205244. doi: 10.1371/journal.pone.0205244. eCollection 2018. PLoS One. 2018. PMID: 30286171 Free PMC article.
-
Biological sex influences psychological aspects of the biopsychosocial model related to chronic pain intensity and interference among South Korean patients with chronic secondary musculoskeletal pain in rheumatic diseases.Front Psychol. 2023 Apr 17;14:1063164. doi: 10.3389/fpsyg.2023.1063164. eCollection 2023. Front Psychol. 2023. PMID: 37138999 Free PMC article.
-
Tactile localization accuracy at the low back.Atten Percept Psychophys. 2024 Apr;86(3):1008-1021. doi: 10.3758/s13414-024-02843-4. Epub 2024 Feb 8. Atten Percept Psychophys. 2024. PMID: 38332382 Free PMC article.
-
Functional cortical changes associated with shoulder instability - a systematic review.Shoulder Elbow. 2022 Aug;14(4):452-464. doi: 10.1177/17585732211019016. Epub 2021 Jun 10. Shoulder Elbow. 2022. PMID: 35846404 Free PMC article.
References
-
- Pleger B, Tegenthoff M, Ragert P, Forster A-F, Dinse HR, Schwenkreis P, Nicolas V, Maier C. Sensorimotor returning in complex regional pain syndrome parallels pain reduction. Ann Neurol. 2005;57(Suppl 3):425–429. - PubMed
-
- Pleger B, Ragert P, Schwenkreis P, Forster A-F, Wilimzig C, Dinse H, Nicolas V, Maier C, Tegenthoff M. Patterns of cortical reorganization parallel impaired tactile discrimination and pain intensity in complex regional syndrome. Neuroimage. 2006;32(Suppl 2):503–510. - PubMed
-
- Moseley L, Flor H. Targeting cortical representations in the treatment of chronic pain: a review. Neurorehabil Neural Repair. 2012;26(Suppl 6):646–652. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
