

Spending of HIV resources in Asia and Eastern Europe: systematic review reveals the need to shift funding allocations towards priority populations
- PMID: 24572053
- PMCID: PMC3936108
- DOI: 10.7448/IAS.17.1.18822
Spending of HIV resources in Asia and Eastern Europe: systematic review reveals the need to shift funding allocations towards priority populations
Abstract
Introduction: It is increasingly important to prioritize the most cost-effective HIV interventions. We sought to summarize the evidence on which types of interventions provide the best value for money in regions with concentrated HIV epidemics.
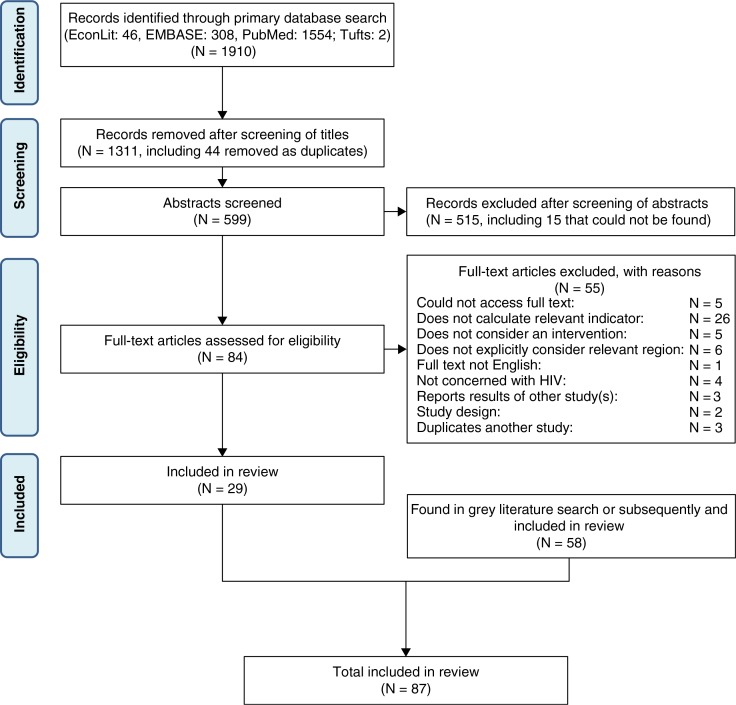
Methods: We conducted a systematic review of peer-reviewed and grey literature reporting measurements of cost-effectiveness or cost-benefit for HIV/AIDS interventions in Asia and Eastern Europe. We also collated HIV/AIDS spending assessment data from case-study countries in the region.
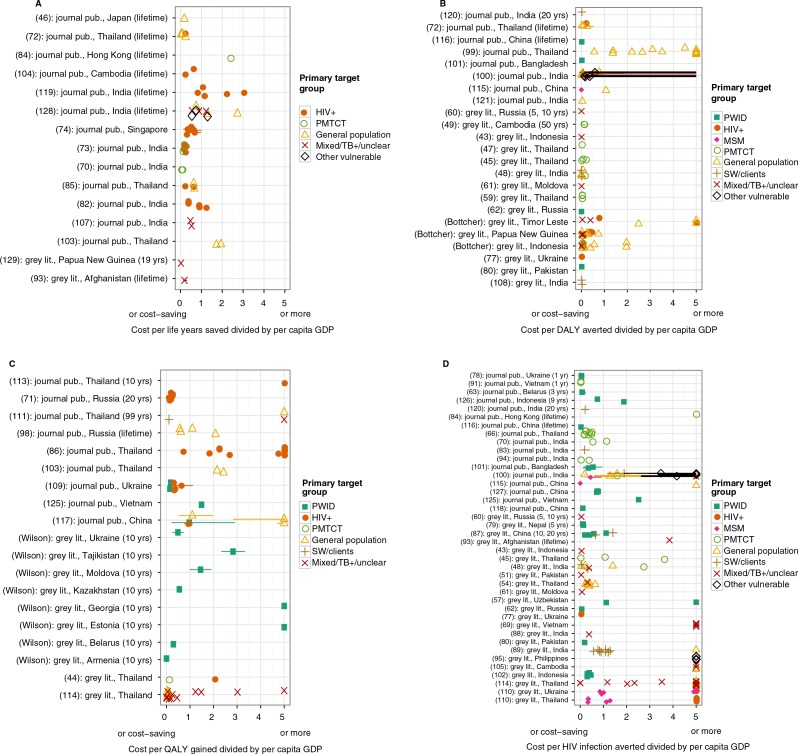
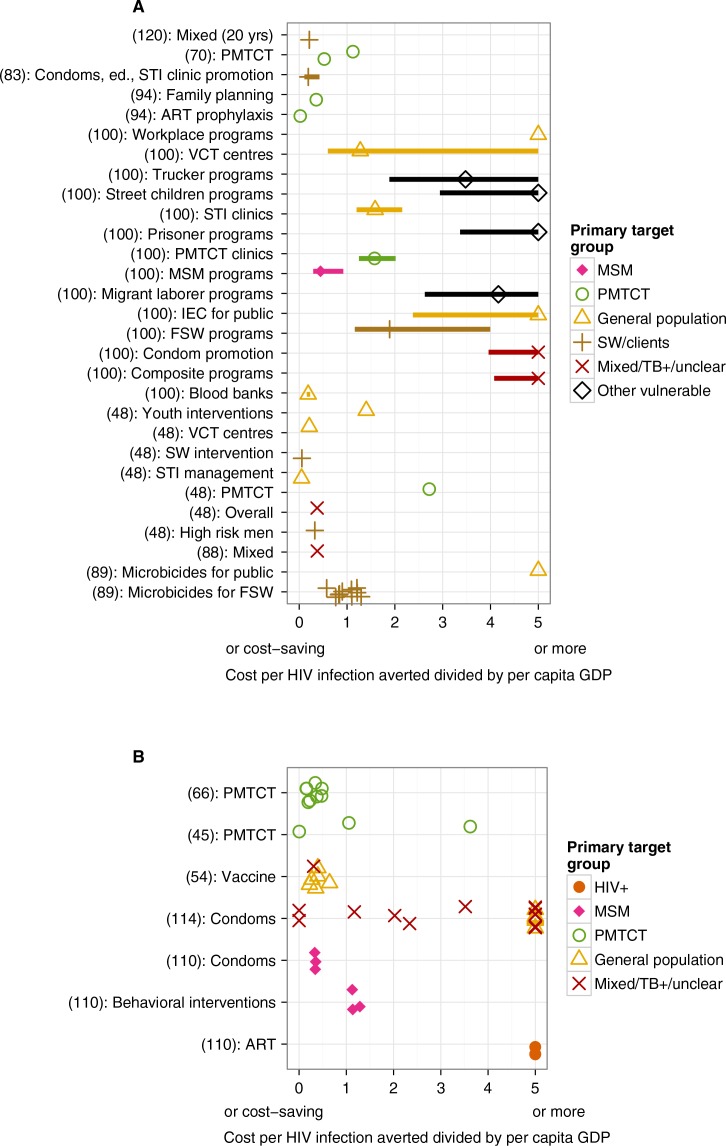
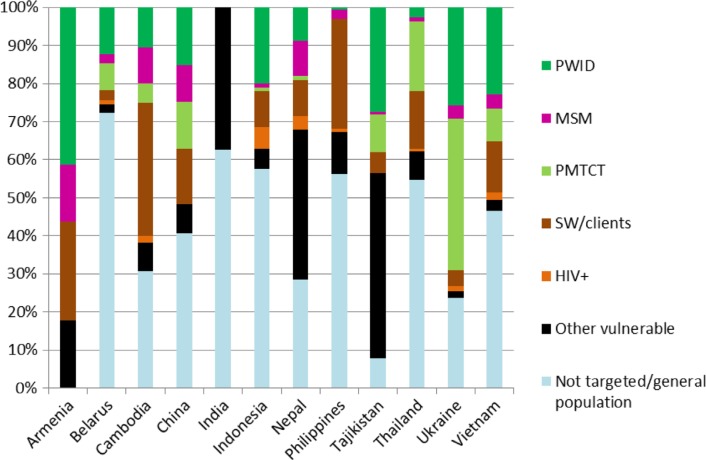
Results: We identified 91 studies for inclusion, 47 of which were from peer-reviewed journals. Generally, in concentrated settings, prevention of mother-to-child transmission programmes and prevention programmes targeting people who inject drugs and sex workers had lower incremental cost-effectiveness ratios than programmes aimed at the general population. The few studies evaluating programmes targeting men who have sex with men indicate moderate cost-effectiveness. Collation of prevention programme spending data from 12 countries in the region (none of which had generalized epidemics) indicated that resources for the general population/non-targeted was greater than 30% for eight countries and greater than 50% for five countries.
Conclusions: There is a misalignment between national spending on HIV/AIDS responses and the most affected populations across the region. In concentrated epidemics, scarce funding should be directed more towards most-at-risk populations. Reaching consensus on general principles of cost-effectiveness of programmes by epidemic settings is difficult due to inconsistent evaluation approaches. Adopting a standard costing, impact evaluation, benefits calculation, analysis and reporting framework would enable cross comparisons and improve HIV resource prioritization and allocation.
Keywords: Asia; Eastern Europe; HIV; concentrated epidemics; cost-benefit analyses; cost-effectiveness; programme evaluation; systematic review.
Figures
References
-
- UNAIDS. UNAIDS World AIDS Day report [Internet]. 2012 [cited 2012 Dec 4] Available from: http://www.unaids.org/en/media/unaids/contentassets/documents/epidemiolo....
-
- Schwartländer B, Stover J, Hallett T, Atun R, Avila C, Gouws E, et al. Towards an improved investment approach for an effective response to HIV/AIDS. Lancet. 2011;377(9782):2031–41. - PubMed
-
- The Global Fund to Fight AIDS, Tuberculosis and Malaria. The Global Fund adopts new strategy to save 10 million lives by 2016 [Internet] The Global Fund to Fight AIDS, Tuberculosis and Malaria; 2011 [cited 2012 Dec 11]. Available from: http://www.theglobalfund.org/en/mediacenter/newsreleases/2011-11-23_The_...
-
- Wolfe D, Carrieri MP, Shepard D. Treatment and care for injecting drug users with HIV infection: a review of barriers and ways forward. Lancet. 2010;376(9738):355–66. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
