

Predictors of clinical improvement in rituximab-treated refractory adult and juvenile dermatomyositis and adult polymyositis
- PMID: 24574235
- PMCID: PMC3987896
- DOI: 10.1002/art.38270
Predictors of clinical improvement in rituximab-treated refractory adult and juvenile dermatomyositis and adult polymyositis
Abstract
Objective: To identify the clinical and laboratory predictors of clinical improvement in a cohort of myositis patients treated with rituximab.
Methods: We analyzed data for 195 patients with myositis (75 with adult polymyositis [PM], 72 with adult dermatomyositis [DM], and 48 with juvenile DM) in the Rituximab in Myositis trial. Clinical improvement was defined as 20% improvement in at least 3 of the following 6 core set measures of disease activity: physician's and patient's/parent's global assessment of disease activity, manual muscle testing, physical function, muscle enzymes, and extramuscular disease activity. We analyzed the association of the following baseline variables with improvement: myositis clinical subgroup, demographics, myositis damage, clinical and laboratory parameters, core set measures, rituximab treatment, and myositis autoantibodies (antisynthetase, anti-Mi-2, anti-signal recognition particle, anti-transcription intermediary factor 1γ [TIF-1γ], anti-MJ, other autoantibodies, and no autoantibodies). All measures were univariately assessed for association with improvement using time-to-event analyses. A multivariable time-dependent proportional hazards model was used to evaluate the association of individual predictive factors with improvement.
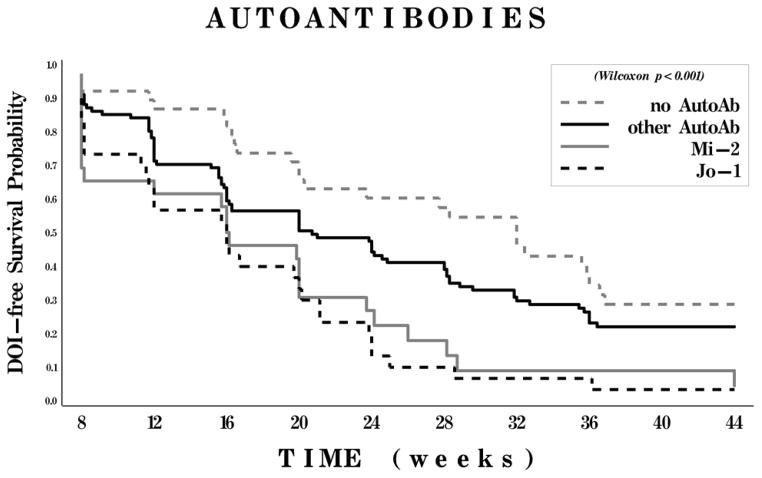
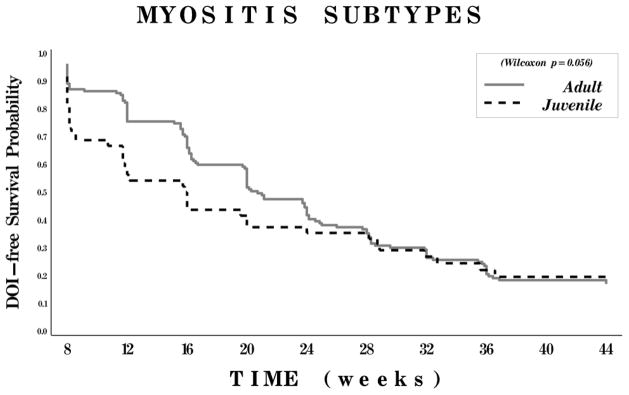
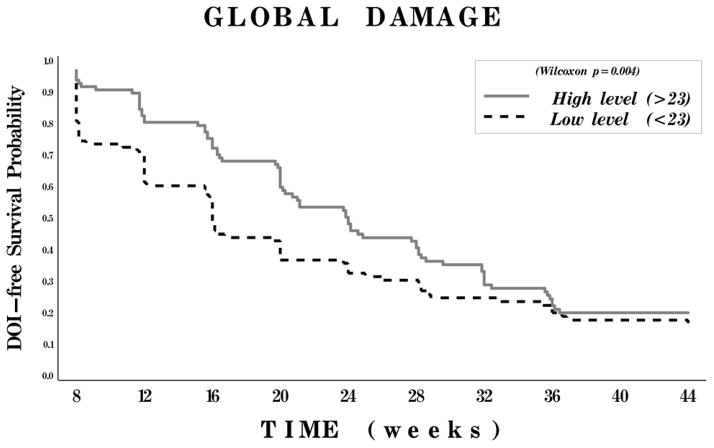
Results: In the final multivariable model, the presence of an antisynthetase, primarily anti-Jo-1 (hazard ratio [HR] 3.08, P < 0.01), anti-Mi-2 (HR 2.5, P < 0.01), or other autoantibody (HR 1.4, P = 0.14) predicted a shorter time to improvement compared to the absence of autoantibodies. A lower physician's global assessment of damage (HR 2.32, P = 0.02) and juvenile DM (versus adult myositis) (HR 2.45, P = 0.01) also predicted improvement. Unlike autoantibody status, the predictive effect of physician's global assessment of damage and juvenile DM diminished by week 20. Rituximab treatment did not affect these associations.
Conclusion: Our findings indicate that the presence of antisynthetase and anti-Mi-2 autoantibodies, juvenile DM subset, and lower disease damage strongly predict clinical improvement in patients with refractory myositis.
Copyright © 2014 by the American College of Rheumatology.
Figures
References
-
- Bohan A, Peter JB. Polymyositis and dermatomyositis (second of two parts) The New England journal of medicine. 1975;292(8):403–7. - PubMed
-
- Bohan A, Peter JB. Polymyositis and dermatomyositis (first of two parts) The New England journal of medicine. 1975;292(7):344–7. - PubMed
-
- Ascherman DP. The role of Jo-1 in the immunopathogenesis of polymyositis: current hypotheses. Current Rheumatol Report. 2003;5(6):425–30. - PubMed
-
- Koga T, Fujikawa K, Horai Y, Okada A, Kawashiri SY, Iwamoto N, et al. The diagnostic utility of anti-melanoma differentiation-associated gene 5 antibody testing for predicting the prognosis of Japanese patients with DM. Rheumatology (Oxford) 2012;51(7):1278–84. - PubMed
-
- Muro Y, Sugiura K, Hoshino K, Akiyama M. Disappearance of anti-MDA-5 autoantibodies in clinically amyopathic DM/interstitial lung disease during disease remission. Rheumatology (Oxford) 2012;51(5):800–4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
