

Asymmetry and heterogeneity of Alzheimer's and frontotemporal pathology in primary progressive aphasia
- PMID: 24574501
- PMCID: PMC3959558
- DOI: 10.1093/brain/awu024
Asymmetry and heterogeneity of Alzheimer's and frontotemporal pathology in primary progressive aphasia
Abstract
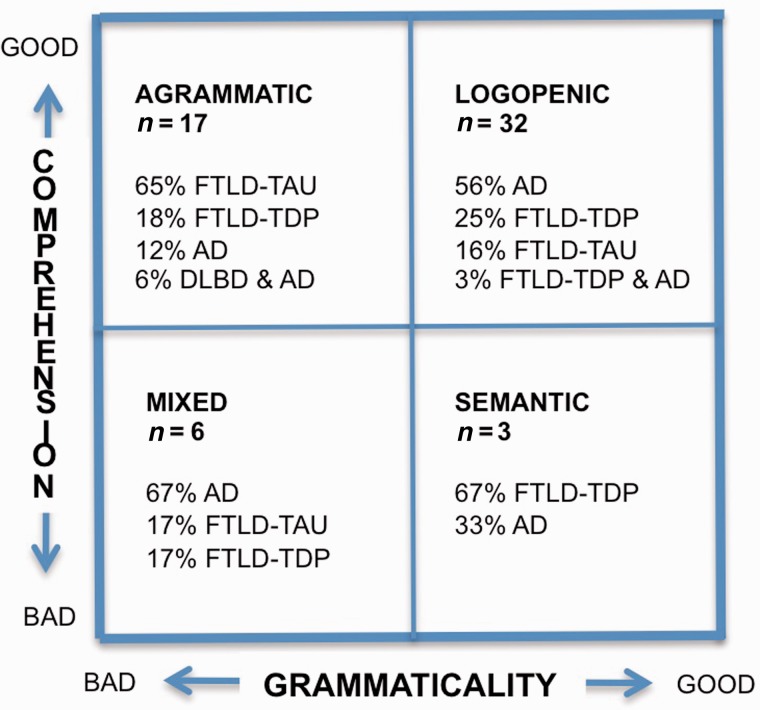
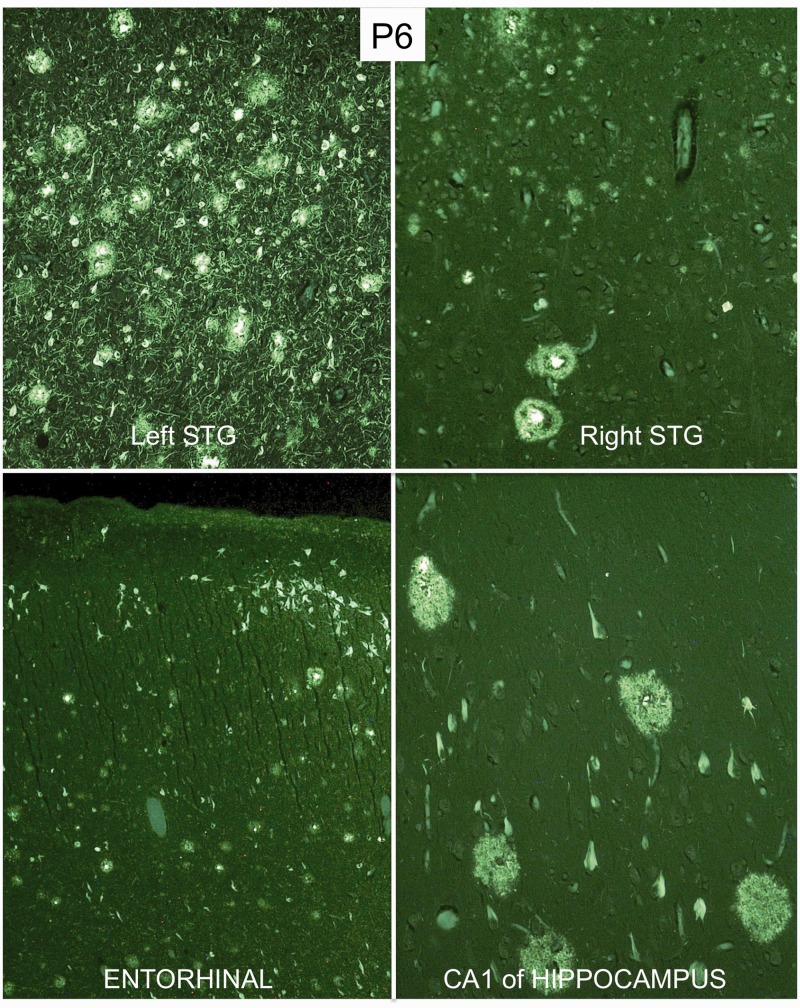
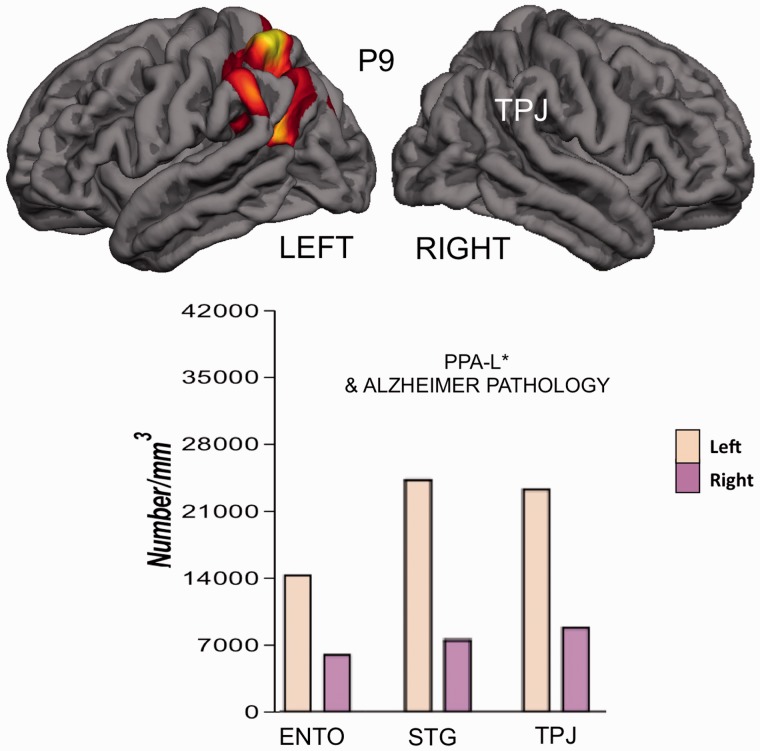
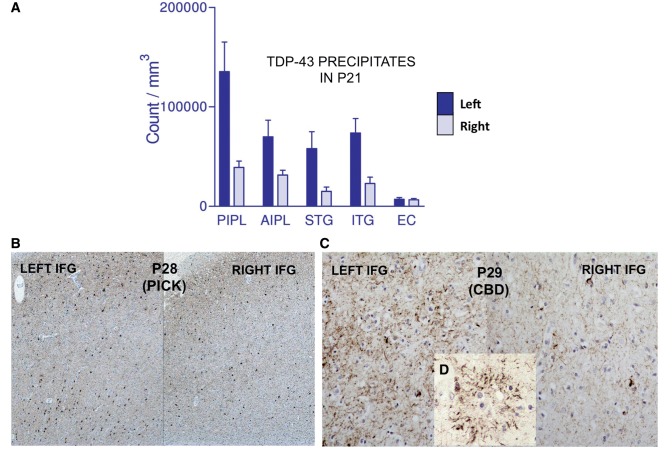
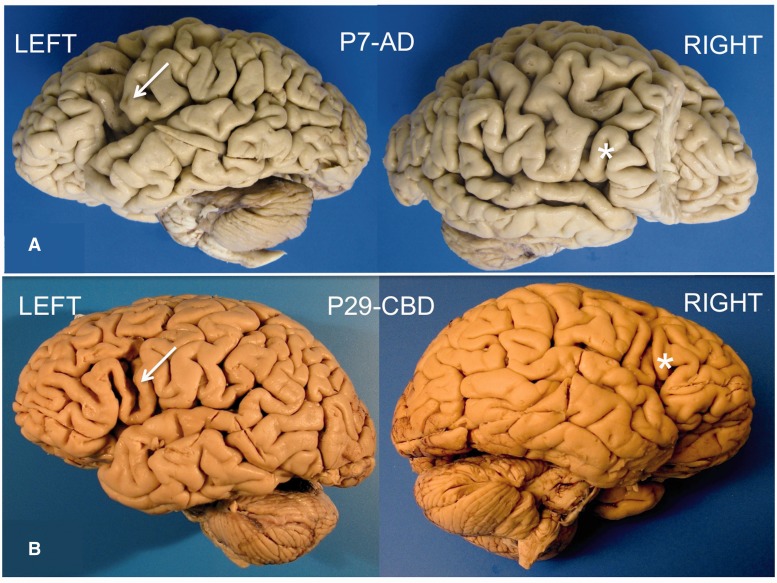
Fifty-eight autopsies of patients with primary progressive aphasia are reported. Twenty-three of these were previously described (Mesulam et al., 2008) but had their neuropathological diagnoses updated to fit current criteria. Thirty-five of the cases are new. Their clinical classification was guided as closely as possible by the 2011 consensus guidelines (Gorno-Tempini et al., 2011). Tissue diagnoses included Alzheimer's disease in 45% and frontotemporal lobar degeneration (FTLD) in the others, with an approximately equal split between TAR DNA binding protein 43 proteinopathies and tauopathies. The most common and distinctive feature for all pathologies associated with primary progressive aphasia was the asymmetric prominence of atrophy, neuronal loss, and disease-specific proteinopathy in the language-dominant (mostly left) hemisphere. The Alzheimer's disease pathology in primary progressive aphasia displayed multiple atypical features. Males tended to predominate, the neurofibrillary pathology was more intense in the language-dominant hemisphere, the Braak pattern of hippocampo-entorhinal prominence was tilted in favour of the neocortex, and the APOE e4 allele was not a risk factor. Mean onset age was under 65 in the FTLD as well as Alzheimer's disease groups. The FTLD-TAR DNA binding protein 43 group had the youngest onset and fastest progression whereas the Alzheimer's disease and FTLD-tau groups did not differ from each other in either onset age or progression rate. Each cellular pathology type had a preferred but not invariant clinical presentation. The most common aphasic manifestation was of the logopenic type for Alzheimer pathology and of the agrammatic type for FTLD-tau. The progressive supranuclear palsy subtype of FTLD-tau consistently caused prominent speech abnormality together with agrammatism whereas FTLD-TAR DNA binding protein 43 of type C consistently led to semantic primary progressive aphasia. The presence of agrammatism made Alzheimer's disease pathology very unlikely whereas the presence of a logopenic aphasia or word comprehension impairment made FTLD-tau unlikely. The association of logopenic primary progressive aphasia with Alzheimer's disease pathology was much more modest than has been implied by results of in vivo amyloid imaging studies. Individual features of the aphasia, such as agrammatism and comprehension impairment, were as informative of underlying pathology as more laborious subtype diagnoses. At the single patient level, no clinical pattern was pathognomonic of a specific neuropathology type, highlighting the critical role of biomarkers for diagnosing the underlying disease. During clinical subtyping, some patients were unclassifiable by the 2011 guidelines whereas others simultaneously fit two subtypes. Revisions of criteria for logopenic primary progressive aphasia are proposed to address these challenges.
Keywords: Alzheimers disease; ApoE e4; aphasia; frontotemporal lobar degeneration; hemispheric lateralization.
Figures

References
-
- Alladi S, Xuereb J, Bak T, Nestor P, Knibb J, Patterson K, et al. Focal cortical presentations of Alzheimer's disease. Brain. 2007;130:2636–45. - PubMed
-
- Caselli RJ, Beach TG, Sue LI, Connor DJ, Sabbagh MN. Progressive aphasia with Lewy bodies. Dement Geriatr Cogn Disord. 2002;14:55–8. - PubMed
-
- Deramecourt V, Lebert F, Debachy B, Mackowiak-Cardoliani MA, Bombois S, Kerdraon O, et al. Prediction of pathology in primary progressive language and speech disorders. Neurology. 2010;74:42–9. - PubMed
-
- Dunn LA, Dunn LM. Peabody picture vocabulary test-4. Minneapolis: Pearson; 2006.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
