

Shunting branch of portal vein and stent position predict survival after transjugular intrahepatic portosystemic shunt
- PMID: 24574750
- PMCID: PMC3921486
- DOI: 10.3748/wjg.v20.i3.774
Shunting branch of portal vein and stent position predict survival after transjugular intrahepatic portosystemic shunt
Abstract
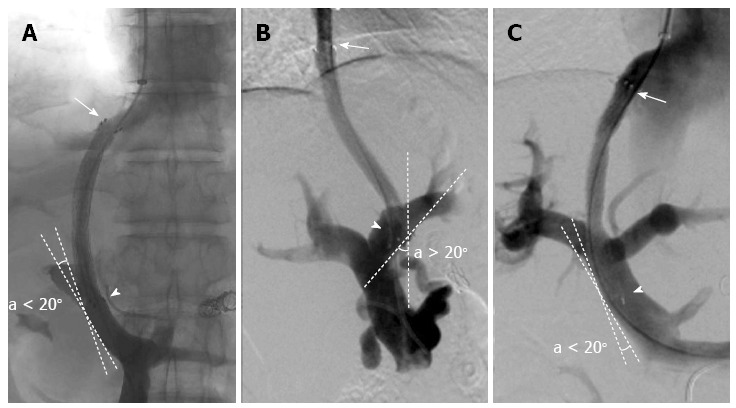
Aim: To evaluate the effect of the shunting branch of the portal vein (PV) (left or right) and the initial stent position (optimal or suboptimal) of a transjugular intrahepatic portosystemic shunt (TIPS).
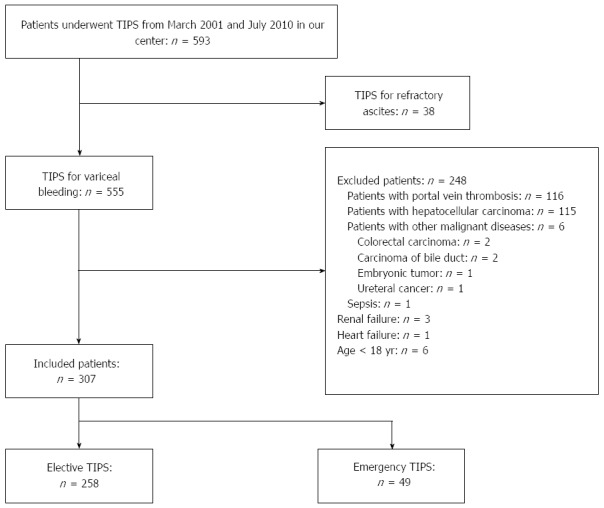
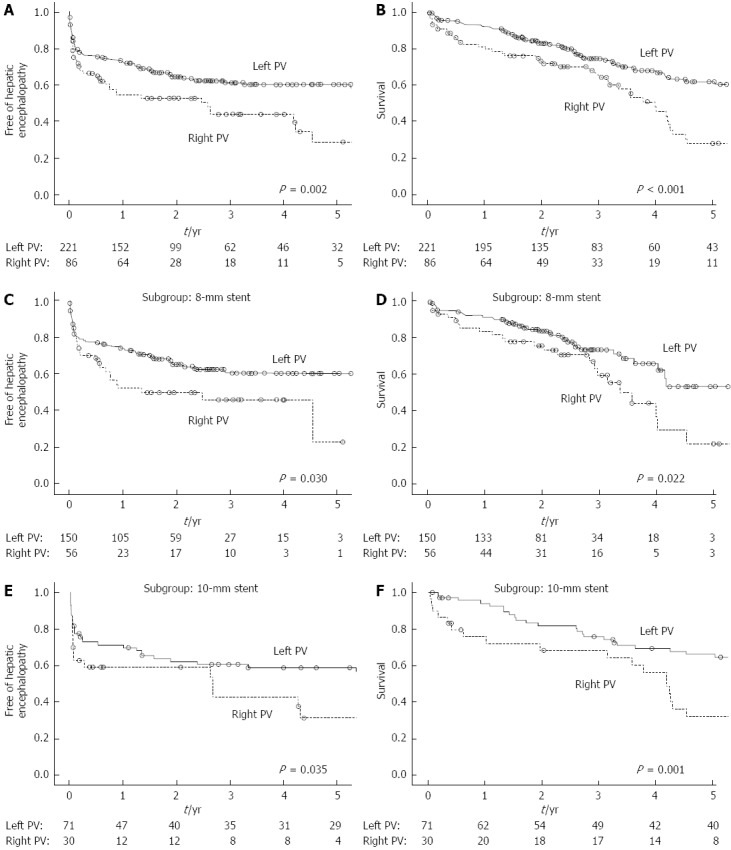
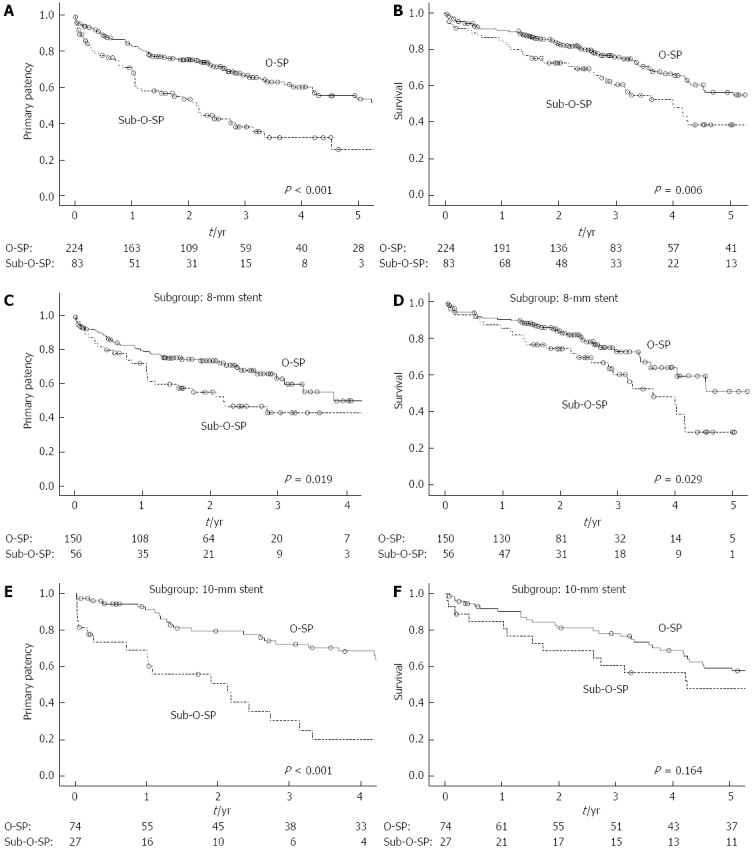
Methods: We retrospectively reviewed 307 consecutive cirrhotic patients who underwent TIPS placement for variceal bleeding from March 2001 to July 2010 at our center. The left PV was used in 221 patients and the right PV in the remaining 86 patients. And, 224 and 83 patients have optimal stent position and sub-optimal stent positions, respectively. The patients were followed until October 2011 or their death. Hepatic encephalopathy, shunt dysfunction, and survival were evaluated as outcomes. The difference between the groups was compared by Kaplan-Meier analysis. A Cox regression model was employed to evaluate the predictors.
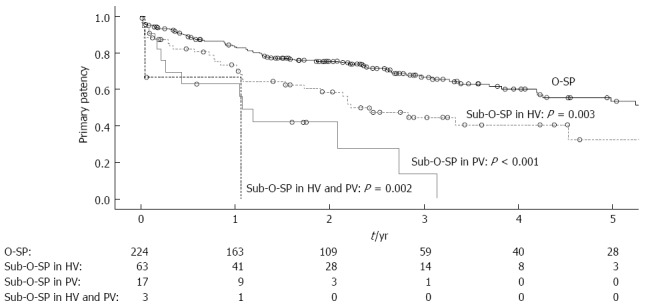
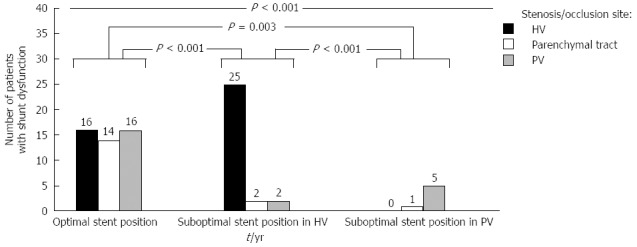
Results: Among the patients who underwent TIPS to the left PV, the risk of hepatic encephalopathy (P = 0.002) and mortality were lower (P < 0.001) compared to those to the right PV. Patients who underwent TIPS with optimal initial stent position had a higher primary patency (P < 0.001) and better survival (P = 0.006) than those with suboptimal initial stent position. The shunting branch of the portal vein and the initial stent position were independent predictors of hepatic encephalopathy and shunt dysfunction after TIPS, respectively. And, both were independent predictors of survival.
Conclusion: TIPS placed to the left portal vein with optimal stent position may reduce the risk of hepatic encephalopathy and improve the primary patency rates, thereby prolonging survival.
Keywords: Cirrhosis; Portal vein; Stent position; Transjugular intrahepatic portosystemic shunt; Variceal bleeding.
Figures
Similar articles
-
Patency of stents covered with polytetrafluoroethylene in patients treated by transjugular intrahepatic portosystemic shunts: long-term results of a randomized multicentre study.Liver Int. 2007 Aug;27(6):742-7. doi: 10.1111/j.1478-3231.2007.01522.x. Liver Int. 2007. PMID: 17617116 Clinical Trial.
-
Effect of technical parameters on transjugular intrahepatic portosystemic shunts utilizing stent grafts.World J Gastroenterol. 2015 Jul 14;21(26):8110-7. doi: 10.3748/wjg.v21.i26.8110. World J Gastroenterol. 2015. PMID: 26185383 Free PMC article.
-
Targeted puncture of left branch of intrahepatic portal vein in transjugular intrahepatic portosystemic shunt to reduce hepatic encephalopathy.World J Gastroenterol. 2019 Mar 7;25(9):1088-1099. doi: 10.3748/wjg.v25.i9.1088. World J Gastroenterol. 2019. PMID: 30862997 Free PMC article.
-
Transjugular intrahepatic portosystemic shunts and portal hypertension-related complications.World J Gastroenterol. 2014 Dec 7;20(45):16996-7010. doi: 10.3748/wjg.v20.i45.16996. World J Gastroenterol. 2014. PMID: 25493012 Free PMC article. Review.
-
The role of transjugular intrahepatic portosystemic shunt (TIPS) in the management of portal hypertension.J Clin Gastroenterol. 2007 Nov-Dec;41 Suppl 3:S344-51. doi: 10.1097/MCG.0b013e318157e500. J Clin Gastroenterol. 2007. PMID: 17975487 Review.
Cited by
-
Safety and efficacy of transjugular intrahepatic portosystemic shunt combined with palliative treatment in patients with hepatocellular carcinoma.World J Clin Cases. 2019 Jul 6;7(13):1599-1610. doi: 10.12998/wjcc.v7.i13.1599. World J Clin Cases. 2019. PMID: 31367619 Free PMC article.
-
Impact of PTFE-covered stent position and extension on TIPS patency.Abdom Radiol (NY). 2020 Nov;45(11):3915-3922. doi: 10.1007/s00261-020-02566-8. Abdom Radiol (NY). 2020. PMID: 32394042
-
The Effect of Puncture Sites of Portal Vein in TIPS with ePTFE-Covered Stents on Postoperative Long-Term Clinical Efficacy.Gastroenterol Res Pract. 2019 Jan 9;2019:2935498. doi: 10.1155/2019/2935498. eCollection 2019. Gastroenterol Res Pract. 2019. PMID: 30728835 Free PMC article.
-
Transjugular intrahepatic portosystemic shunt placement: portal vein puncture guided by 3D/2D image registration of contrast-enhanced multi-detector computed tomography and fluoroscopy.Abdom Radiol (NY). 2020 Nov;45(11):3934-3943. doi: 10.1007/s00261-020-02589-1. Abdom Radiol (NY). 2020. PMID: 32451673 Free PMC article.
-
Clinical efficacy of transjugular intrahepatic portosystemic shunt in the treatment of hepatopulmonary syndrome.Medicine (Baltimore). 2017 Dec;96(49):e9080. doi: 10.1097/MD.0000000000009080. Medicine (Baltimore). 2017. PMID: 29245324 Free PMC article.
References
-
- Rössle M, Deibert P, Haag K, Ochs A, Olschewski M, Siegerstetter V, Hauenstein KH, Geiger R, Stiepak C, Keller W, et al. Randomised trial of transjugular-intrahepatic-portosystemic shunt versus endoscopy plus propranolol for prevention of variceal rebleeding. Lancet. 1997;349:1043–1049. - PubMed
-
- García-Pagán JC, Caca K, Bureau C, Laleman W, Appenrodt B, Luca A, Abraldes JG, Nevens F, Vinel JP, Mössner J, Bosch J. Early use of TIPS in patients with cirrhosis and variceal bleeding. N Engl J Med. 2010;362:2370–2379. - PubMed
-
- Boyer TD, Haskal ZJ. The Role of Transjugular Intrahepatic Portosystemic Shunt (TIPS) in the Management of Portal Hypertension: update 2009. Hepatology. 2010;51:306. - PubMed
-
- European Association for the Study of the Liver. EASL clinical practice guidelines on the management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome in cirrhosis. J Hepatol. 2010;53:397–417. - PubMed
-
- Cello JP, Ring EJ, Olcott EW, Koch J, Gordon R, Sandhu J, Morgan DR, Ostroff JW, Rockey DC, Bacchetti P, et al. Endoscopic sclerotherapy compared with percutaneous transjugular intrahepatic portosystemic shunt after initial sclerotherapy in patients with acute variceal hemorrhage. A randomized, controlled trial. Ann Intern Med. 1997;126:858–865. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
