

Renal adverse effects of sunitinib and its clinical significance: a single-center experience in Korea
- PMID: 24574832
- PMCID: PMC3932394
- DOI: 10.3904/kjim.2014.29.1.40
Renal adverse effects of sunitinib and its clinical significance: a single-center experience in Korea
Abstract
Background/aims: Sunitinib is an oral multitargeted tyrosine kinase inhibitor used mainly for the treatment of metastatic renal cell carcinoma. The renal adverse effects (RAEs) of sunitinib have not been investigated. The aim of this study was to determine the incidence and risk factors of RAEs (proteinuria [PU] and renal insufficiency [RI]) and to investigate the relationship between PU and antitumor efficacy.
Methods: We performed a retrospective review of medical records of patients who had received sunitinib for more than 3 months.
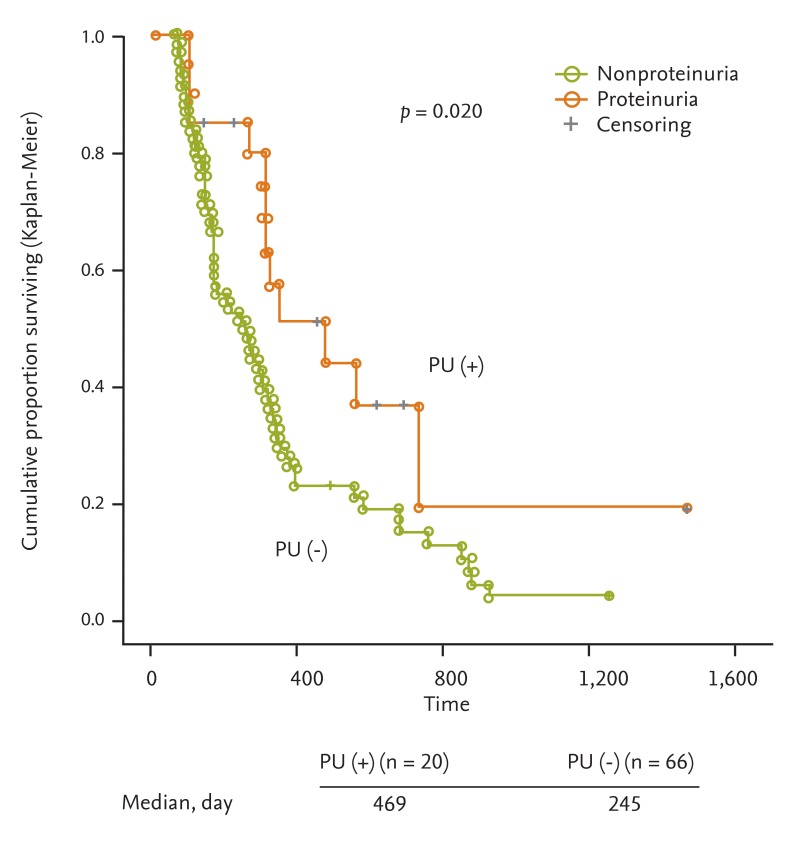
Results: One hundred and fifty-five patients (mean age, 58.7 ± 12.6 years) were enrolled, and the mean baseline creatinine level was 1.24 mg/dL. PU developed in 15 of 111 patients, and preexisting PU was aggravated in six of 111 patients. Only one patient developed typical nephrotic syndrome. Following discontinuation of sunitinib, PU was improved in 12 of 17 patients but persisted in five of 17 patients. RI occurred in 12 of 155 patients, and the maximum creatinine level was 3.31 mg/dL. RI improved in two of 12 patients but persisted in 10 of 12 patients. Risk factors for PU were hypertension, dyslipidemia, and chronic kidney disease. Older age was a risk factor for RI. The median progression-free survival was significantly better for patients who showed PU.
Conclusions: The incidence of RAEs associated with sunitinib was lower than those of previous reports. The severity of RAEs was mild to moderate, and partially reversible after cessation of sunitinib. We suggest that blood pressure, urinalysis, and renal function in patients receiving sunitinib should be monitored closely.
Keywords: Acute kidney injury; Proteinuria; Sunitinib.
Conflict of interest statement
No potential conflict of interest relevant to this article is reported.
Figures
Comment in
-
Risks associated with sunitinib use and monitoring to improve patient outcomes.Korean J Intern Med. 2014 Jan;29(1):23-6. doi: 10.3904/kjim.2014.29.1.23. Epub 2014 Jan 2. Korean J Intern Med. 2014. PMID: 24574829 Free PMC article. No abstract available.
References
-
- Boehm S, Rothermundt C, Hess D, Joerger M. Antiangiogenic drugs in oncology: a focus on drug safety and the elderly: a mini-review. Gerontology. 2010;56:303–309. - PubMed
-
- Gurevich F, Perazella MA. Renal effects of anti-angiogenesis therapy: update for the internist. Am J Med. 2009;122:322–328. - PubMed
-
- Oudard S, Beuselinck B, Decoene J, Albers P. Sunitinib for the treatment of metastatic renal cell carcinoma. Cancer Treat Rev. 2011;37:178–184. - PubMed
-
- Rini BI, Garcia JA, Cooney MM, et al. Toxicity of sunitinib plus bevacizumab in renal cell carcinoma. J Clin Oncol. 2010;28:e284–e285. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources