

Efficacy of a new video-based training model in spinal surgery
- PMID: 24575316
- PMCID: PMC3927092
- DOI: 10.4103/2152-7806.124973
Efficacy of a new video-based training model in spinal surgery
Abstract
Background: An important part of neurosurgical training is the improvement of surgical skills. Acquiring microsurgical skills follows a learning curve, influenced by specific exercises, feedback, and training. Aim of training should be rapid learning success. The study shows the way in which video-based training can influence the learning curve.
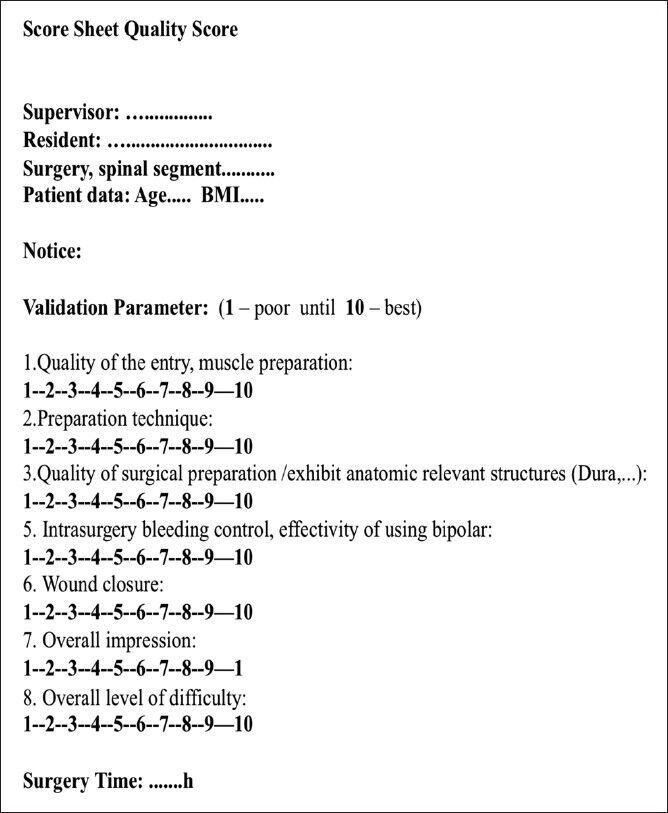
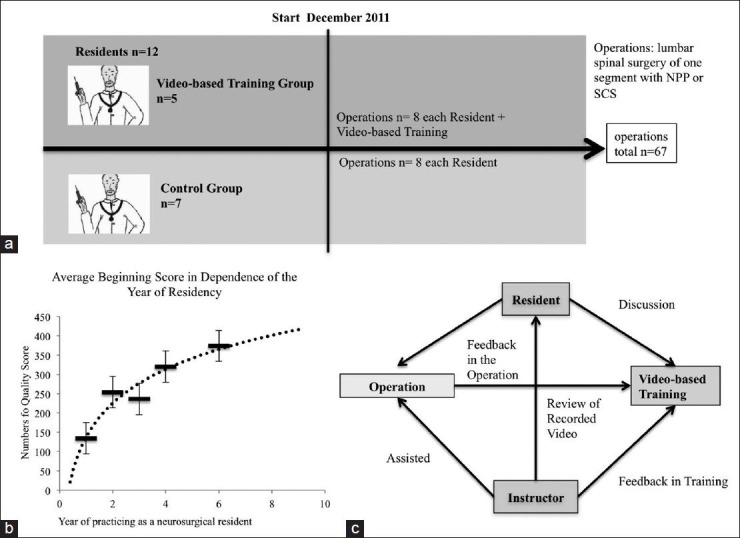
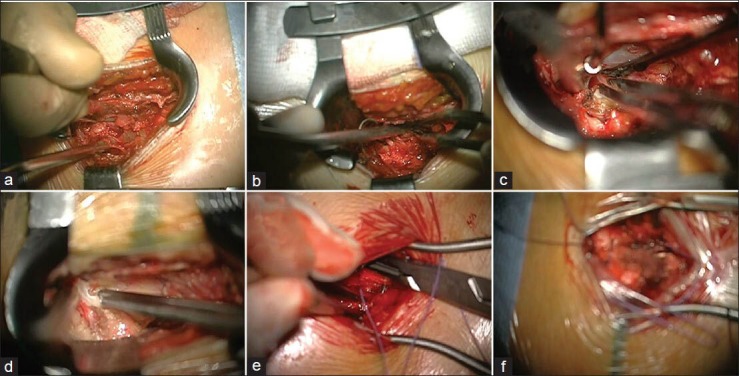
Methods: Over a period of 18 months (2011-2012) 12 residents were evaluated in spinal surgery (12 cases per resident) by a skilled evaluator based on different criteria. The evaluation criteria (exposition of important anatomy, intraoperative bleeding, efficacy of using bipolar cauterization) were weighted and added to a single quality-score. The participating residents were divided into two groups. Only one group (n = 5) received video-based training.
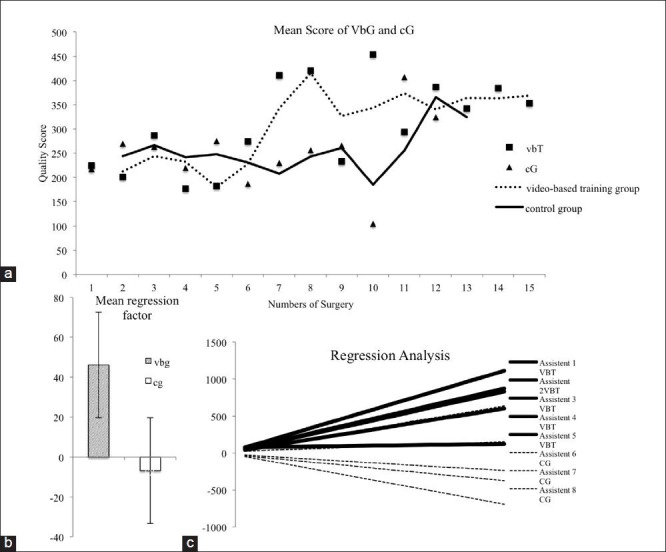
Results: Residents showed an individually different but explicit increase in microsurgical skills. The quality-score during the first surgery compared with the end point of the study demonstrated a faster improvement of surgical skills in the group with video-based training than in the group without special training. Considering all residents together, the video-training group displayed a steeper gradient of microsurgical success. Comparison of the single resident's microsurgical skills showed individual disparities. Various biases that influence the learning success are under examination.
Conclusion: Video-based training can improve microsurgical skills, leading to an improved learning curve. An earlier entry of the learning curve plateau in the video-training group promotes a higher acquisition of surgical skills. Because of the positive effect, we plan to apply the video-based training model to other neurosurgical subspecialties, especially neurovascular and skull base surgery.
Keywords: Learning curve; microsurgery; surgical skills; video-based training.
Figures
References
-
- Buchmann P, Dinçler S. Learning curve-calculation and value in laparoscopic surgery. Ther Umsch. 2005;62:69–75. - PubMed
-
- Chan WY, Figus A, Ekwobi C, Srinivasan JR, Ramakrishnan VV. The ‘round-the-clock’ training model for assessment and warm up of microsurgical skills: A validation study. J Plast Reconstr Aesthet Surg. 2010;63:1323–8. - PubMed
-
- Lascar I, Totir D, Cinca A, Cortan S, Stefanescu A, Bratianu R, et al. Training program and learning curve in experimental microsurgery during the residency in plastic surgery. Microsurgery. 2007;27:263–7. - PubMed
-
- Neudert M, Kluge A, Beleites T, Kemper M, Zahnert T. Microsurgical skills training with a new tympanoplasty model: Learning curve and motivational impact. Otol Neurotol. 2012;33:364–70. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
