

Phase 1 results of safety and tolerability in a rush oral immunotherapy protocol to multiple foods using Omalizumab
- PMID: 24576338
- PMCID: PMC3936817
- DOI: 10.1186/1710-1492-10-7
Phase 1 results of safety and tolerability in a rush oral immunotherapy protocol to multiple foods using Omalizumab
Abstract
Background: Up to 30% of patients with food allergies have clinical reactivity to more than one food allergen. Although there is currently no cure, oral immunotherapy (OIT) is under investigation. Pilot data have shown that omalizumab may hasten the ability to tolerate over 4 g of food allergen protein.
Objective: To evaluate the safety and dose tolerability of a Phase 1 Single Site OIT protocol using omalizumab to allow for a faster and safe desensitization to multiple foods simultaneously.
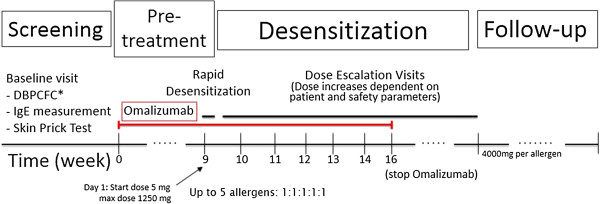
Methods: Participants with multiple food allergies received OIT for up to 5 allergens simultaneously with omalizumab (rush mOIT). Omalizumab was administered for 8 weeks prior to and 8 weeks following the initiation of a rush mOIT schedule. Home reactions were recorded with diaries.
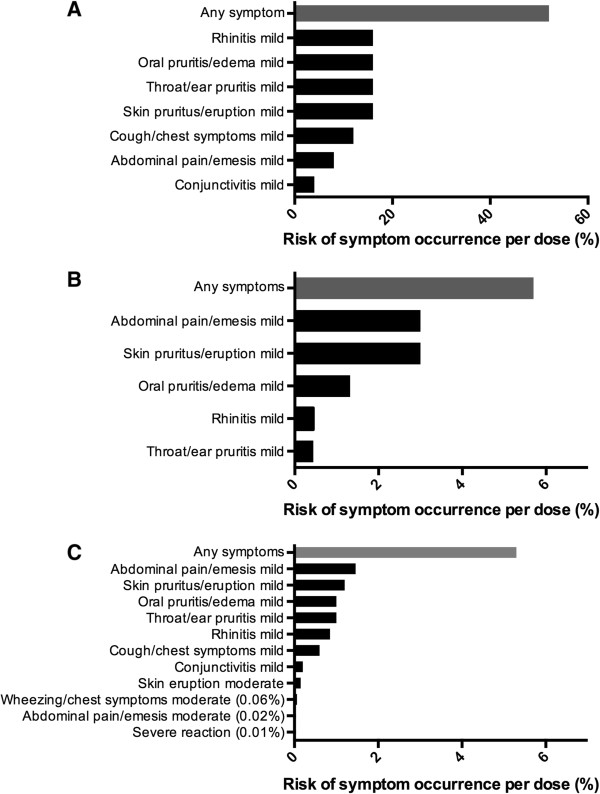
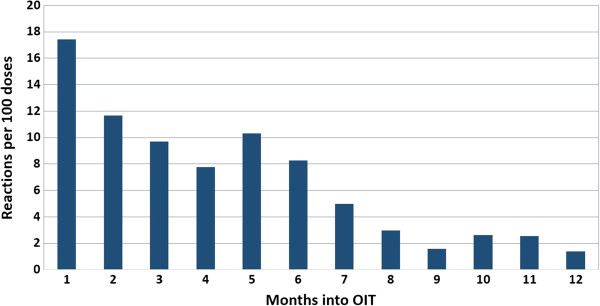
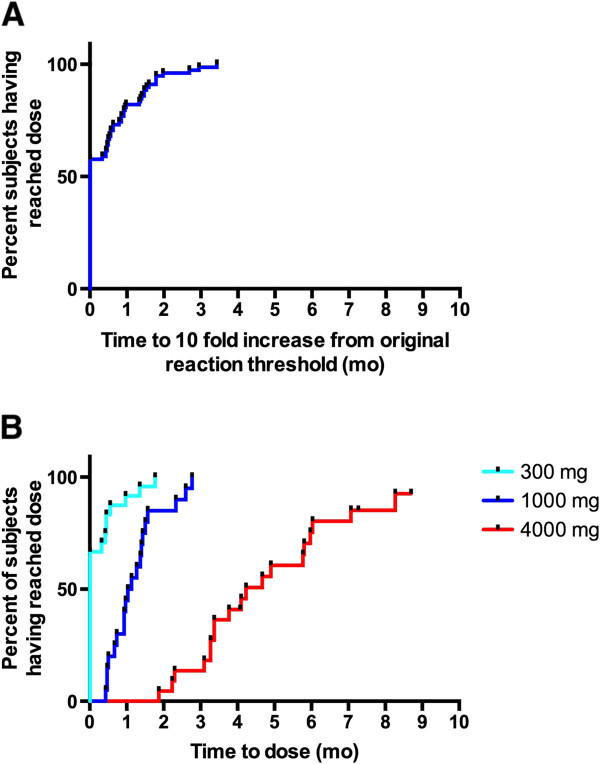
Results: Twenty-five (25) participants were enrolled in the protocol (median age 7 years). For each included food, participants had failed an initial double-blind placebo-controlled food challenge at a protein dose of 100 mg or less. After pre-treatment with omalizumab, 19 participants tolerated all 6 steps of the initial escalation day (up to 1250 mg of combined food proteins), requiring minimal or no rescue therapy. The remaining 6 were started on their highest tolerated dose as their initial daily home doses. Participants reported 401 reactions per 7,530 home doses (5.3%) with a median of 3.2 reactions per 100 doses. Ninety-four percent (94%) of reactions were mild. There was one severe reaction. Participants reached their maintenance dose of 4,000 mg protein per allergen at a median of 18 weeks.
Conclusion: These phase 1 data demonstrate that rush OIT to multiple foods with 16 weeks of treatment with omalizumab could allow for a fast desensitization in subjects with multiple food allergies. Phase 2 randomized controlled trials are needed to better define safety and efficacy parameters of multi OIT experimental treatments with and without omalizumab.
Figures
References
-
- Gupta R, Holdford D, Bilaver L, Dyer A, Holl JL, Meltzer D. The economic impact of childhood food allergy in the United States. JAMA Pediatr. 2013;137(11) - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
