

Impact of human papilloma virus infection on the response of head and neck cancers to anti-epidermal growth factor receptor antibody therapy
- PMID: 24577089
- PMCID: PMC3944273
- DOI: 10.1038/cddis.2014.62
Impact of human papilloma virus infection on the response of head and neck cancers to anti-epidermal growth factor receptor antibody therapy
Abstract
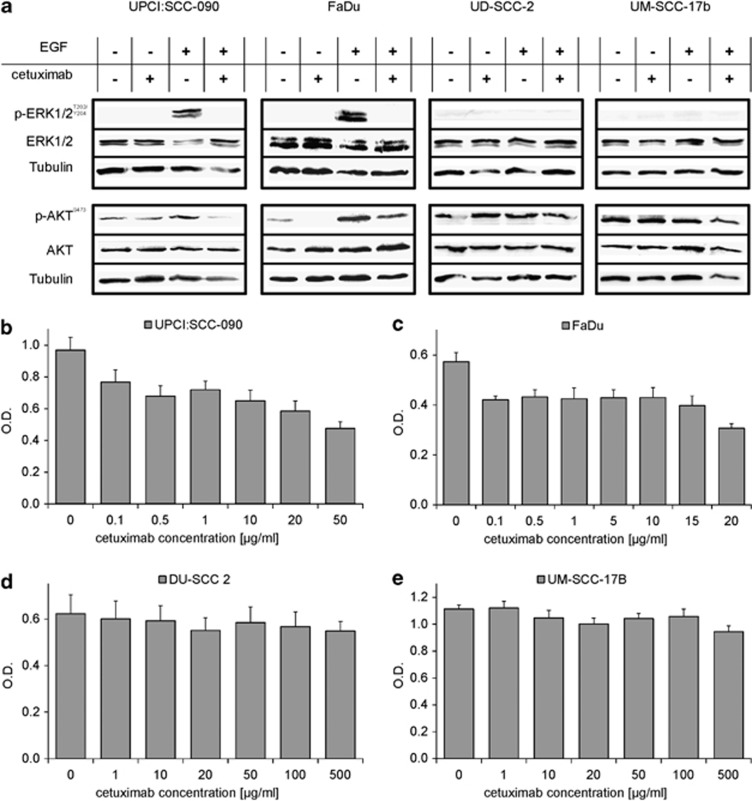
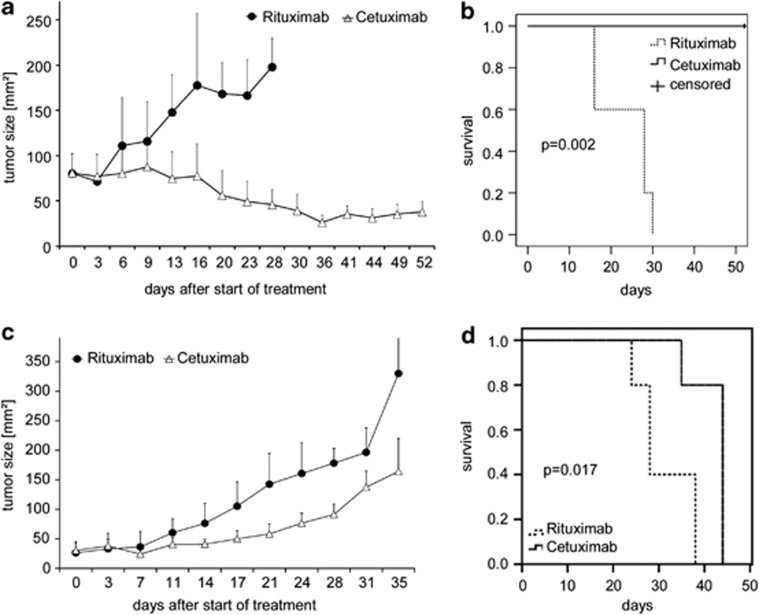
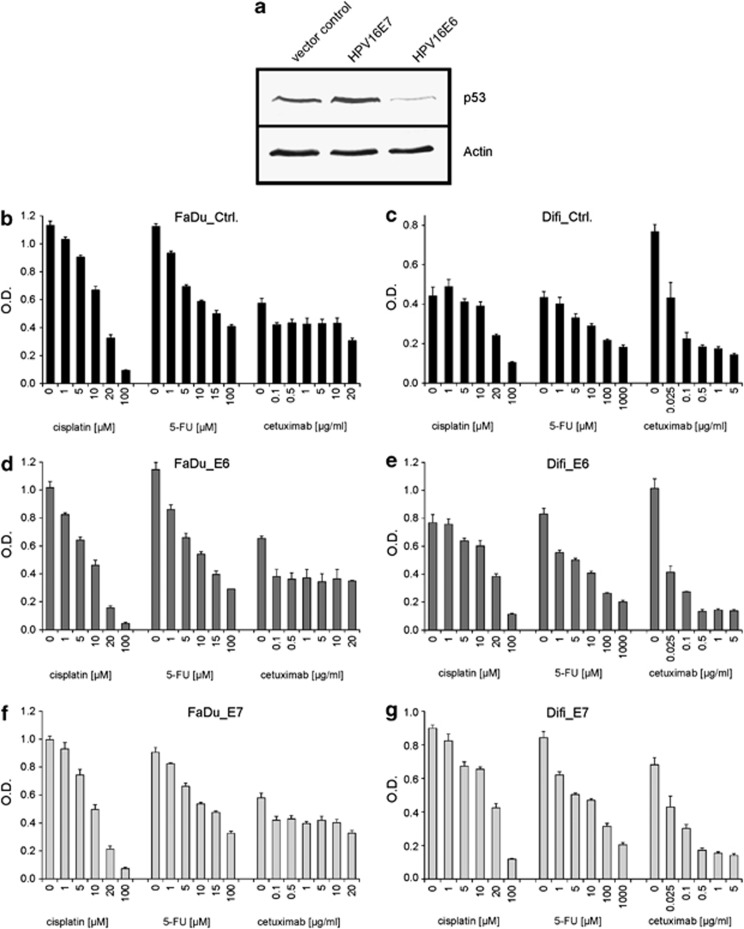
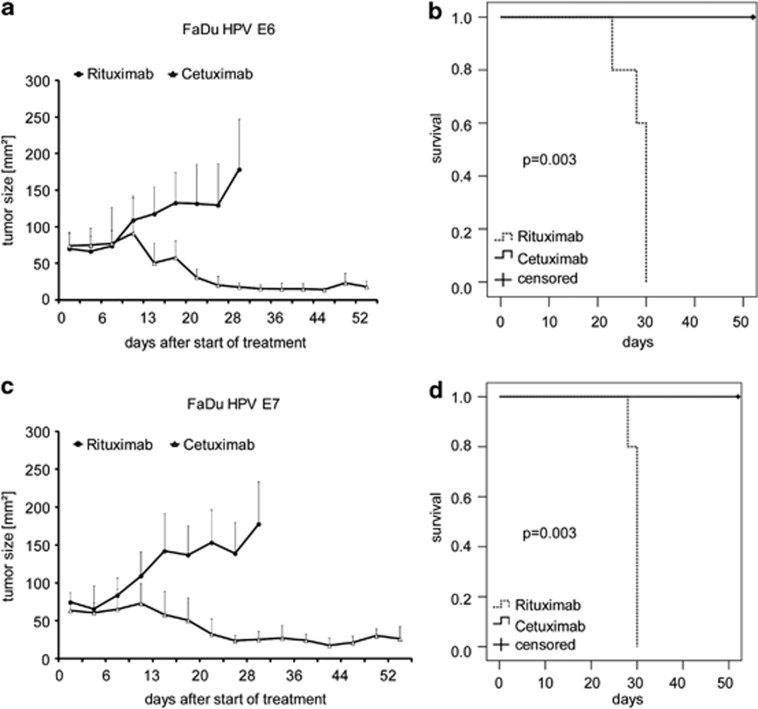
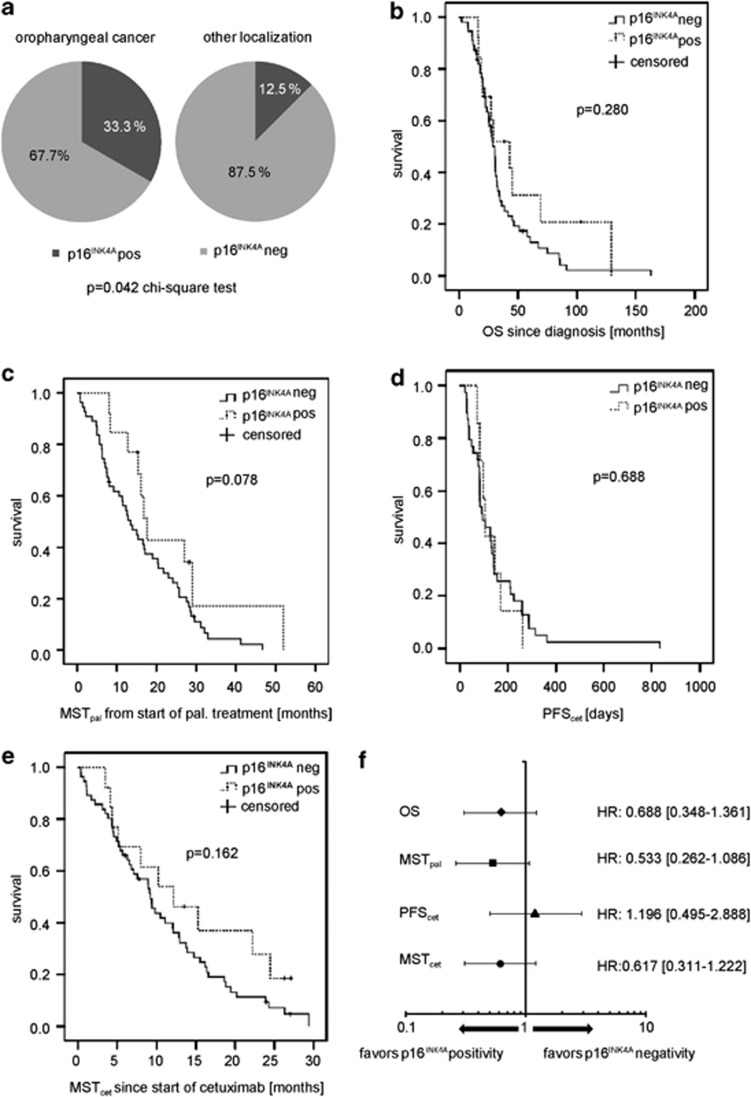
Infection with human papillomaviruses (HPVs) characterizes a distinct subset of head and neck squamous cell cancers (HNSCCs). HPV-positive HNSCC preferentially affect the oropharynx and tonsils. Localized HPV-positive HNSCCs have a favorable prognosis and treatment outcome. However, the impact of HPV in advanced or metastatic HNSCC remains to be defined. In particular, it is unclear whether HPV modulates the response to cetuximab, an antibody targeting the epidermal growth factor receptor (EGFR), which is a mainstay of treatment of advanced HNSCC. To this end, we have examined the sensitivity of HPV-positive and -negative HNSCC models to cetuximab and cytotoxic drugs in vitro and in vivo. In addition, we have stably expressed the HPV oncogenes E6 and E7 in cetuximab-sensitive cancer cell lines to specifically investigate their role in the antibody response. The endogenous HPV status or the expression of HPV oncogenes had no significant impact on cetuximab-mediated suppression of EGFR signaling and proliferation in vitro. Cetuximab effectively inhibited the growth of E6- and E7-expressing tumors grafted in NOD/SCID mice. In support, formalin-fixed, paraffin-embedded tumor samples from cetuximab-treated patients with recurrent or metastatic HNSCC were probed for p16(INK4a) expression, an established biomarker of HPV infection. Response rates (45.5% versus 45.5%) and median progression-free survival (97 versus 92 days) following cetuximab-based therapy were similar in patients with p16(INK4A)-positive and p16(INK4A)-negative tumors. In conclusion, HPV oncogenes do not modulate the anti-EGFR antibody response in HSNCC. Cetuximab treatment should be administered independently of HPV status.
Figures
References
-
- Leemans CR, Braakhuis BJ, Brakenhoff RH. The molecular biology of head and neck cancer. Nat Rev Cancer. 2011;11:9–22. - PubMed
-
- Hong AM, Grulich AE, Jones D, Lee CS, Garland SM, Dobbins TA, et al. Squamous cell carcinoma of the oropharynx in Australian males induced by human papillomavirus vaccine targets. Vaccine. 2010;28:3269–3272. - PubMed
-
- Mork J, Lie AK, Glattre E, Hallmans G, Jellum E, Koskela P, et al. Human papillomavirus infection as a risk factor for squamous-cell carcinoma of the head and neck. N Engl J Med. 2001;344:1125–1131. - PubMed
-
- Nasman A, Attner P, Hammarstedt L, Du J, Eriksson M, Giraud G, et al. Incidence of human papillomavirus (HPV) positive tonsillar carcinoma in Stockholm, Sweden: an epidemic of viral-induced carcinoma. Int J Cancer. 2009;125:362–366. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
