

Reset of a critically disturbed microbial ecosystem: faecal transplant in recurrent Clostridium difficile infection
- PMID: 24577353
- PMCID: PMC4817604
- DOI: 10.1038/ismej.2014.13
Reset of a critically disturbed microbial ecosystem: faecal transplant in recurrent Clostridium difficile infection
Abstract
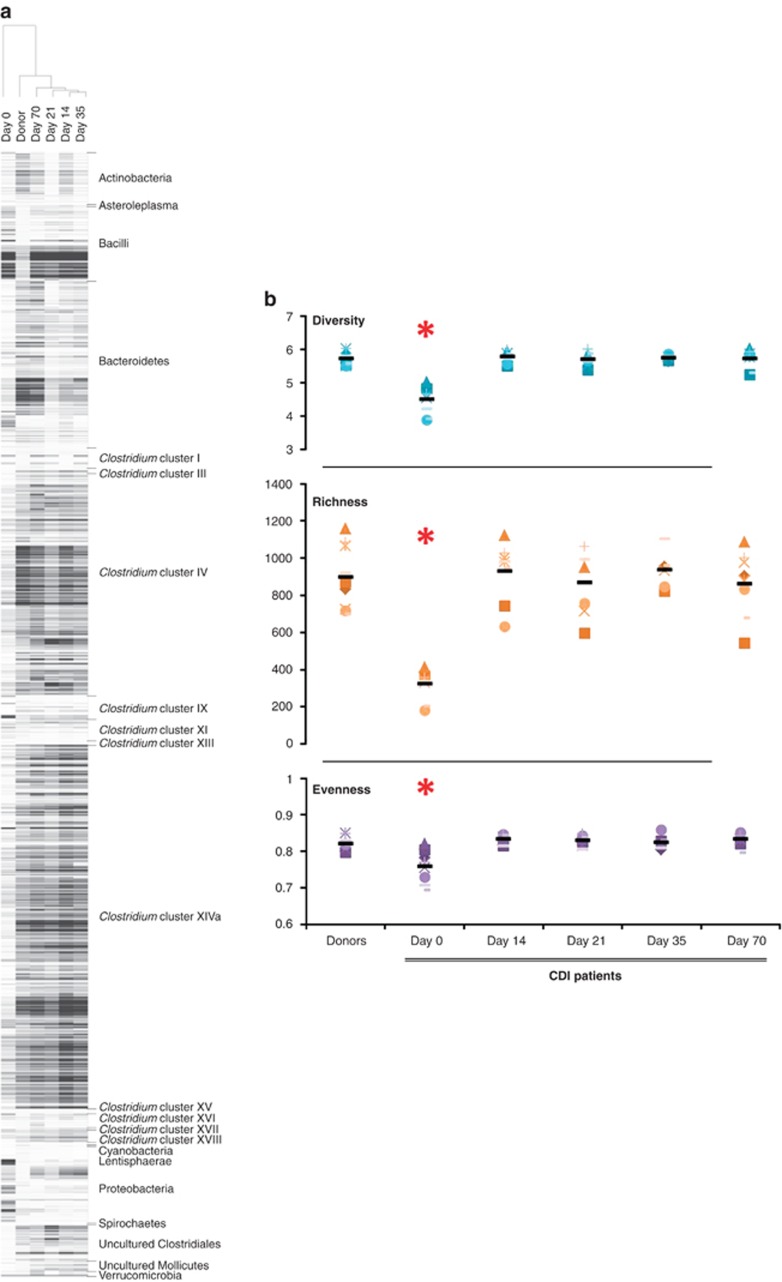
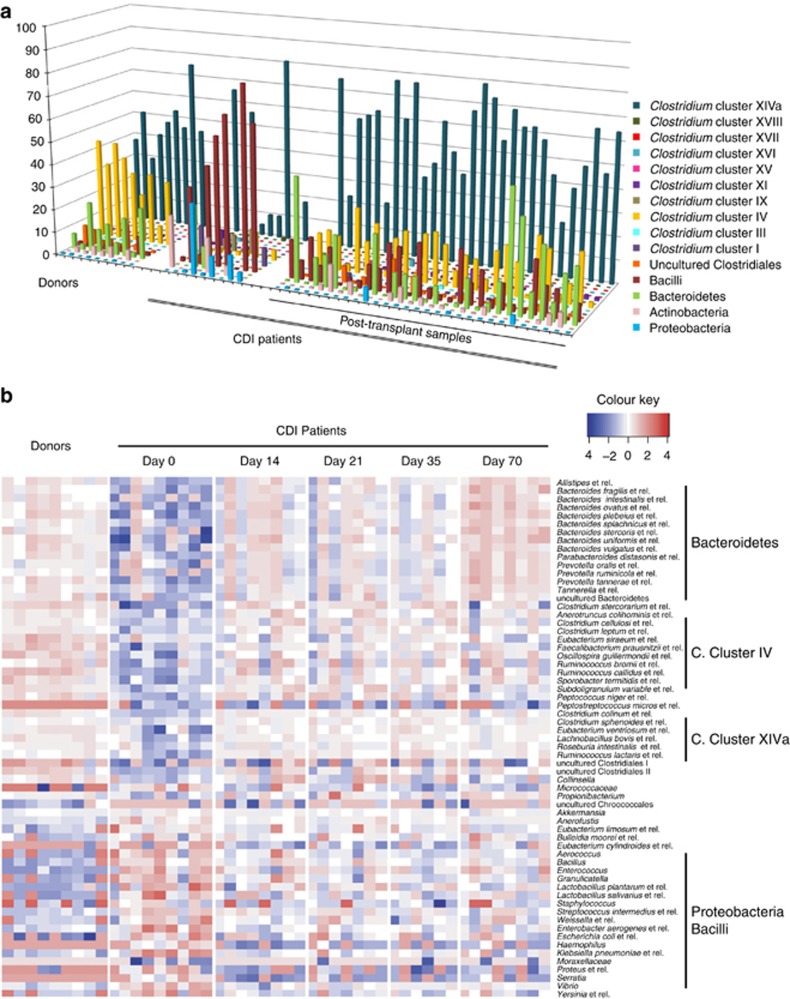
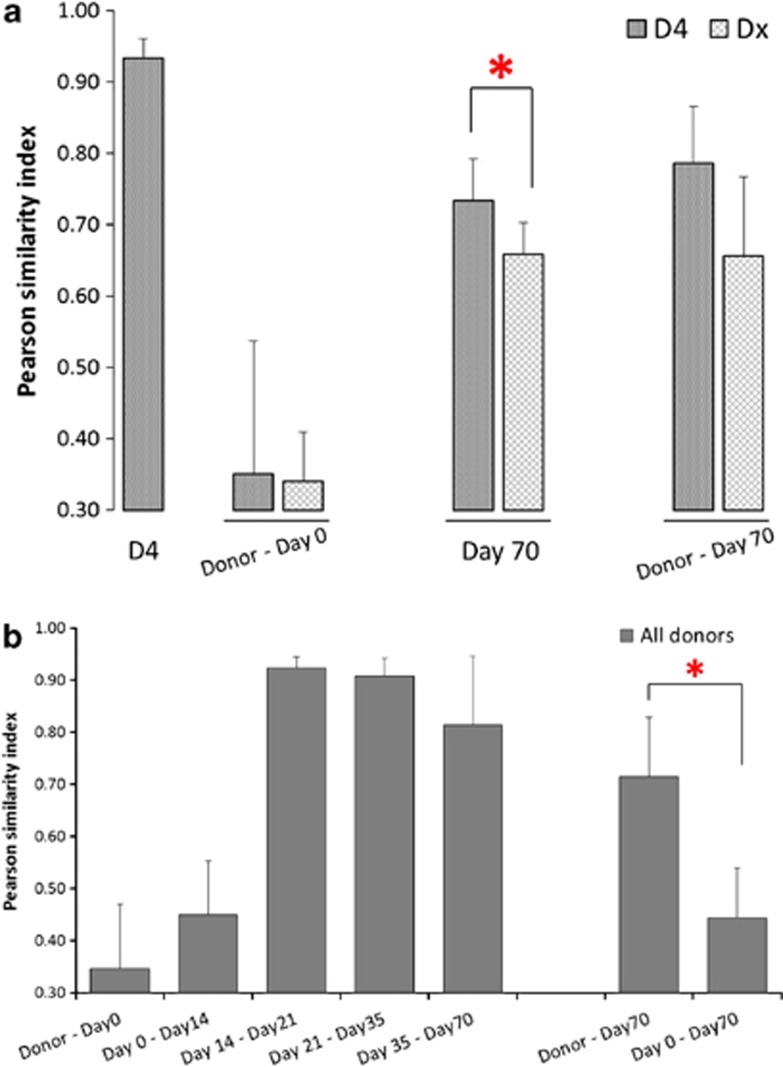
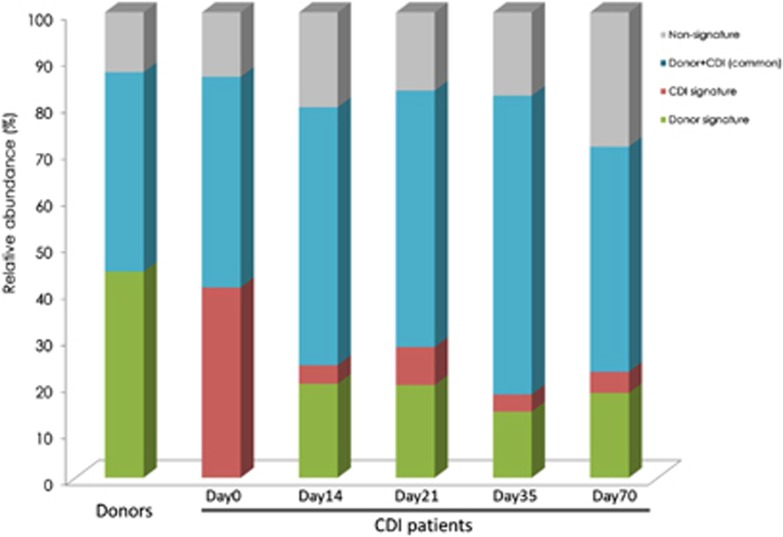
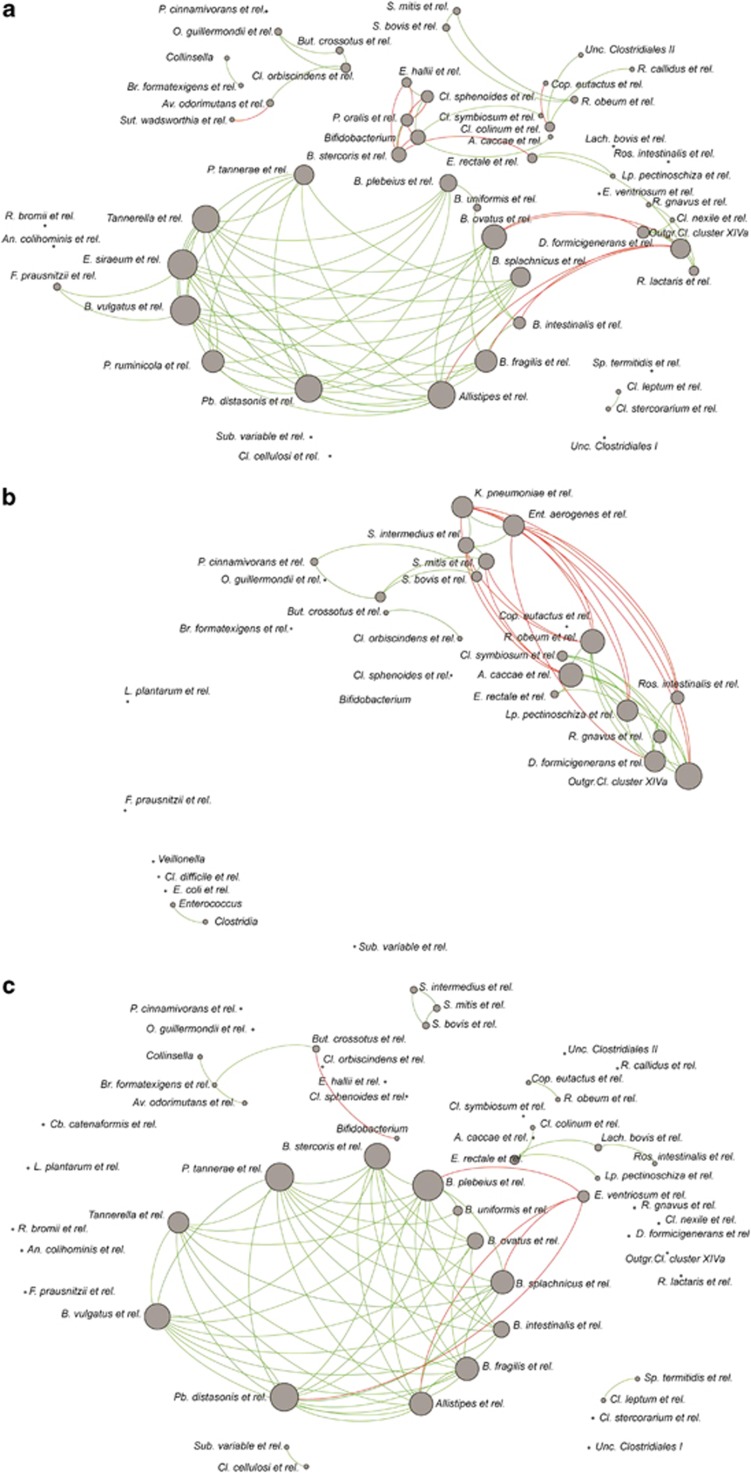
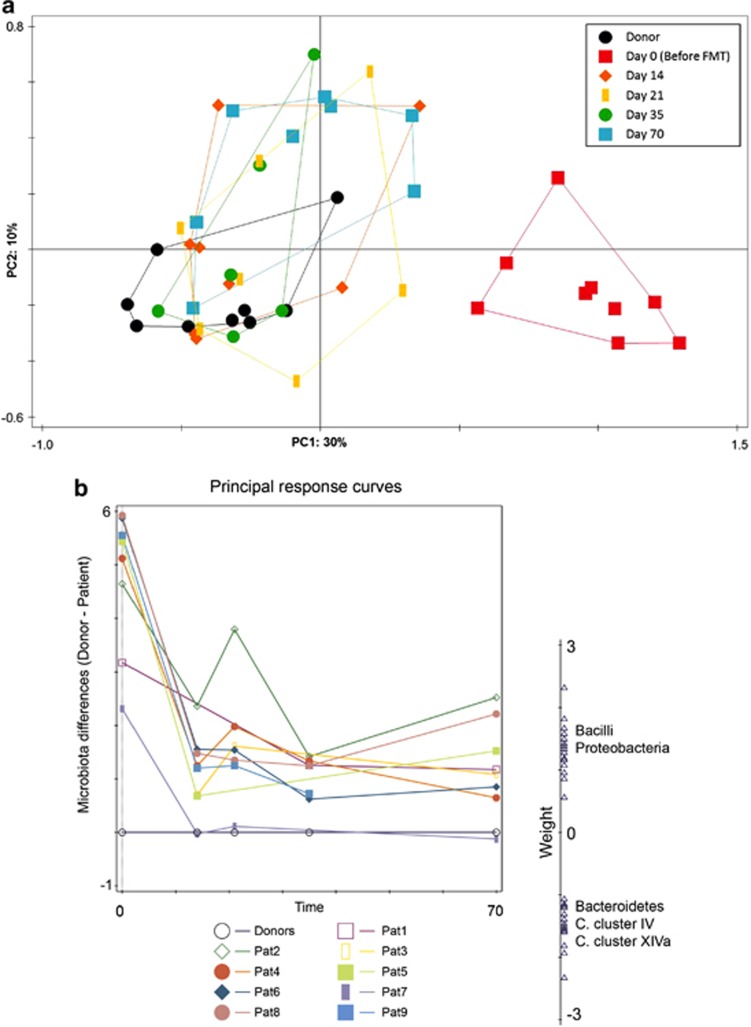
Recurrent Clostridium difficile infection (CDI) can be effectively treated by infusion of a healthy donor faeces suspension. However, it is unclear what factors determine treatment efficacy. By using a phylogenetic microarray platform, we assessed composition, diversity and dynamics of faecal microbiota before, after and during follow-up of the transplantation from a healthy donor to different patients, to elucidate the mechanism of action of faecal infusion. Global composition and network analysis of the microbiota was performed in faecal samples from nine patients with recurrent CDI. Analyses were performed before and after duodenal donor faeces infusion, and during a follow-up of 10 weeks. The microbiota data were compared with that of the healthy donors. All patients successfully recovered. Their intestinal microbiota changed from a low-diversity diseased state, dominated by Proteobacteria and Bacilli, to a more diverse ecosystem resembling that of healthy donors, dominated by Bacteroidetes and Clostridium groups, including butyrate-producing bacteria. We identified specific multi-species networks and signature microbial groups that were either depleted or restored as a result of the treatment. The changes persisted over time. Comprehensive and deep analyses of the microbiota of patients before and after treatment exposed a therapeutic reset from a diseased state towards a healthy profile. The identification of microbial groups that constitute a niche for C. difficile overgrowth, as well as those driving the reinstallation of a healthy intestinal microbiota, could contribute to the development of biomarkers predicting recurrence and treatment outcome, identifying an optimal microbiota composition that could lead to targeted treatment strategies.
Figures
References
-
- Ananthakrishnan AN, Issa M, Binion DG. (2009). Clostridium difficile and inflammatory bowel disease. Gastroenterol Clin North Am 38: 711–728. - PubMed
-
- Aziz Q, Doré J, Emmanuel A, Guarner F, Quigley EMM. (2013). Gut microbiota and gastrointestinal health: current concepts and future directions. Neurogastroenterol Motil 25: 4–15. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
