

Radiation dosimetry and first therapy results with a (124)I/ (131)I-labeled small molecule (MIP-1095) targeting PSMA for prostate cancer therapy
- PMID: 24577951
- PMCID: PMC4052014
- DOI: 10.1007/s00259-014-2713-y
Radiation dosimetry and first therapy results with a (124)I/ (131)I-labeled small molecule (MIP-1095) targeting PSMA for prostate cancer therapy
Abstract
Introduction: Since the prostate-specific membrane antigen (PSMA) is frequently over-expressed in prostate cancer (PCa) several PSMA-targeting molecules are under development to detect and treat metastatic castration resistant prostate cancer (mCRPC). We investigated the tissue kinetics of a small molecule inhibitor of PSMA ((S)-2-(3-((S)-1-carboxy-5-(3-(4-[(124)I]iodophenyl)ureido)pentyl)ureido)pentanedioicacid; MIP-1095) using PET/CT to estimate radiation dosimetry for the potential therapeutic use of (131)I-MIP-1095 in men with mCRPC. We also report preliminary safety and efficacy of the first 28 consecutive patients treated under a compassionate-use protocol with a single cycle of (131)I-MIP-1095.
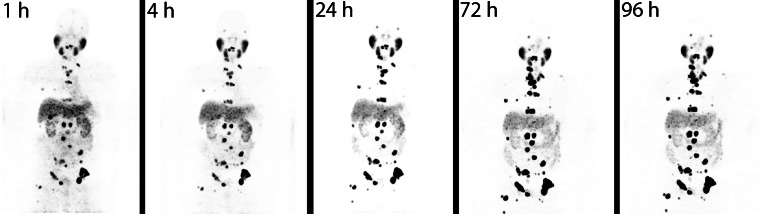
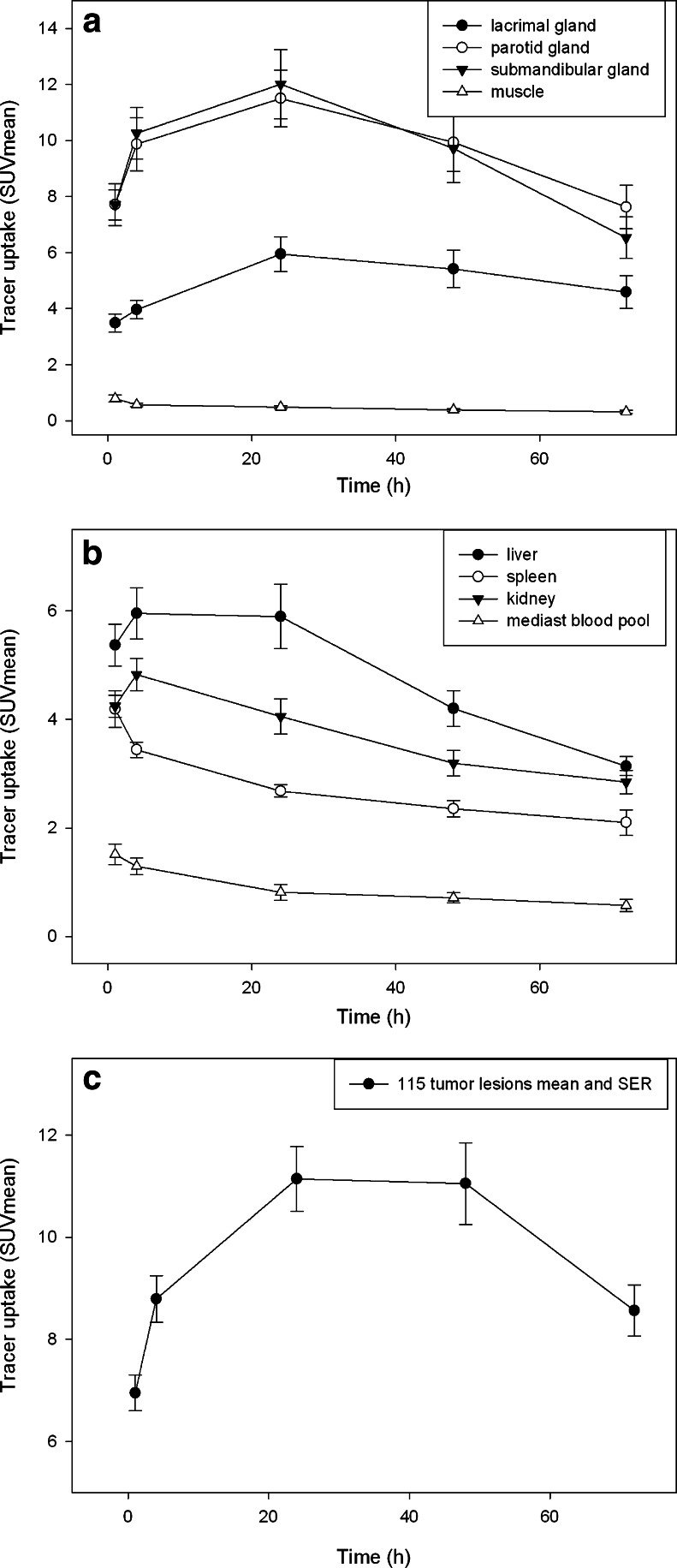
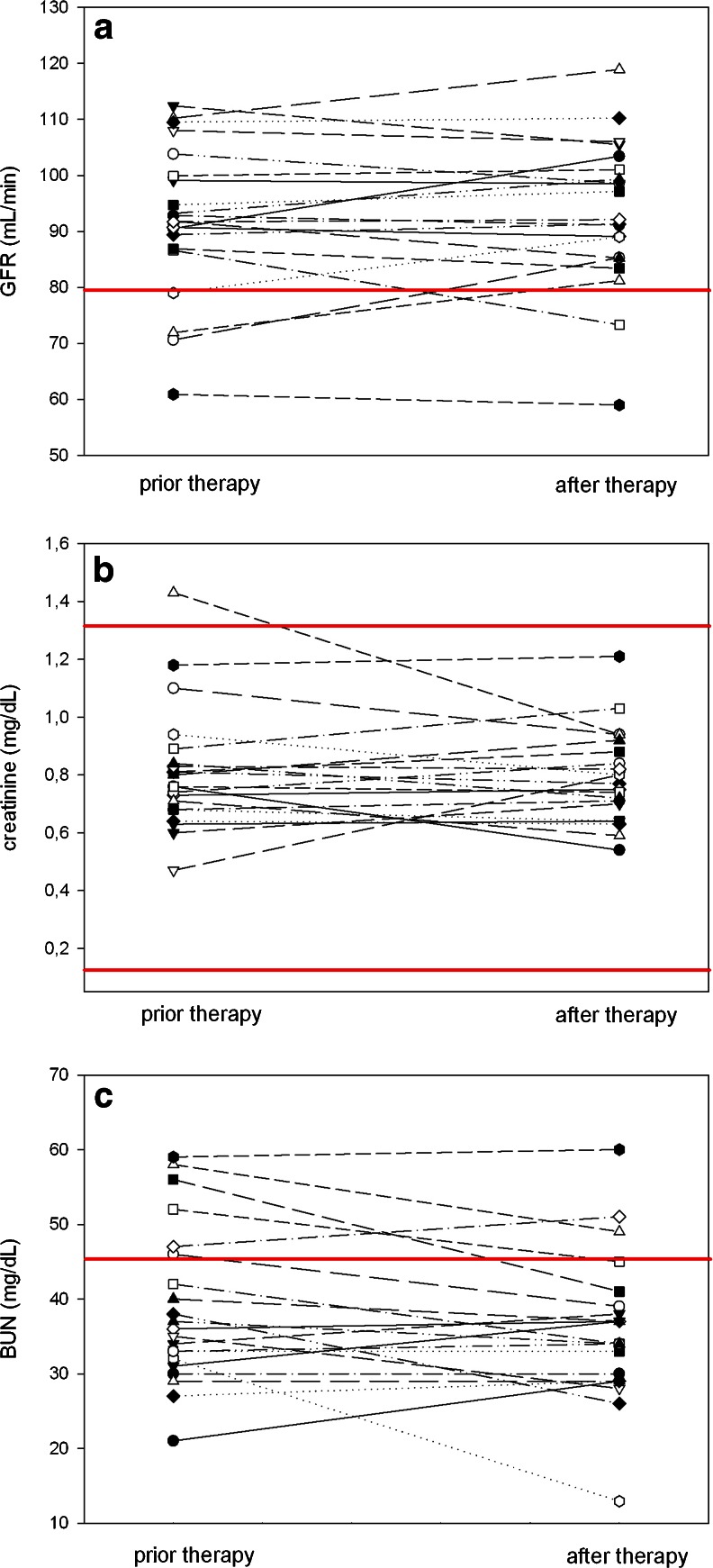
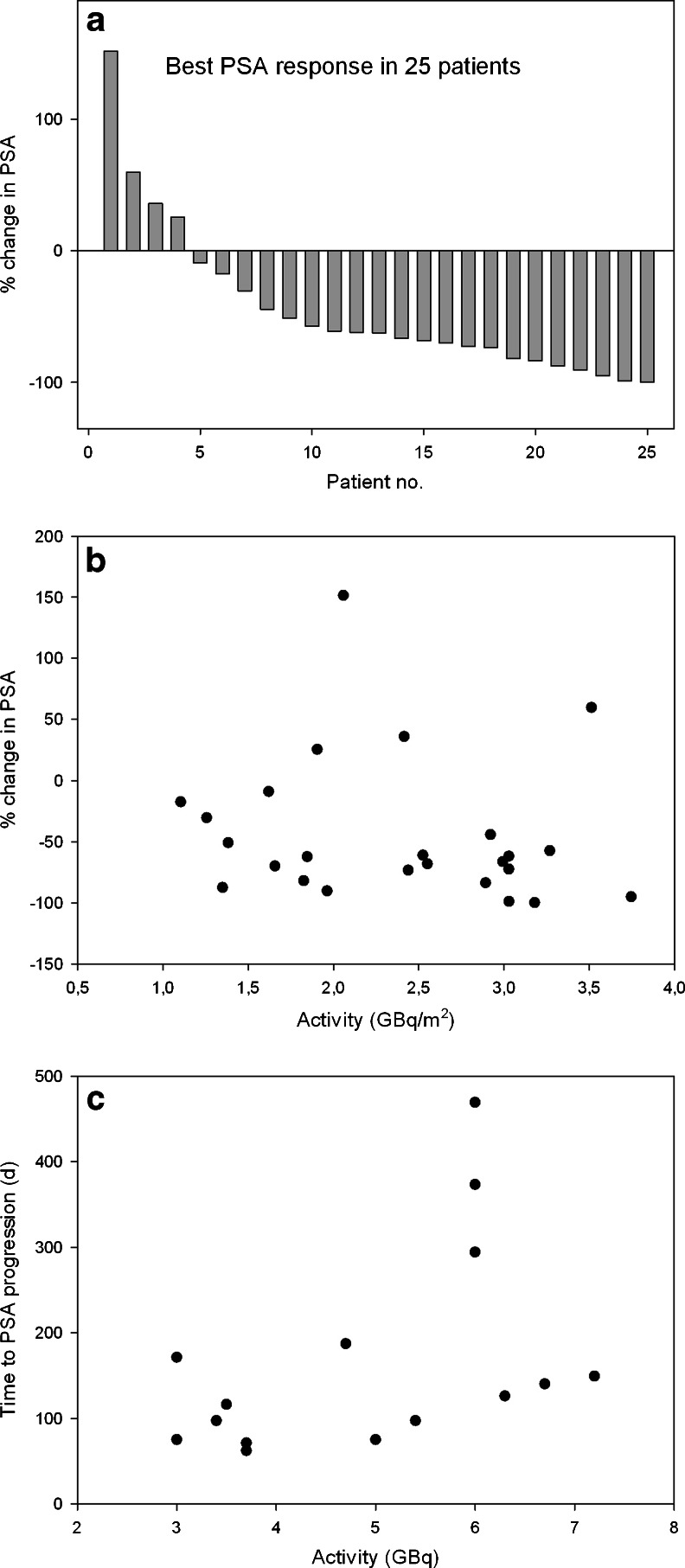
Methods: Sixteen patients with known prostate cancer underwent PET/CT imaging after i.v. administration of (124)I-MIP-1095 (mean activity: 67.4 MBq). Each patient was scanned using PET/CT up to five times at 1, 4, 24, 48 and 72 h post injection. Volumes of interest were defined for tumor lesions and normal organs at each time point followed by dose calculations using the OLINDA/EXM software. Twenty-eight men with mCRPC were treated with a single cycle of (131)I-MIP-1095 (mean activity: 4.8 GBq, range 2 to 7.2 GBq) and followed for safety and efficacy. Baseline and follow up examinations included a complete blood count, liver and kidney function tests, and measurement of serum PSA.
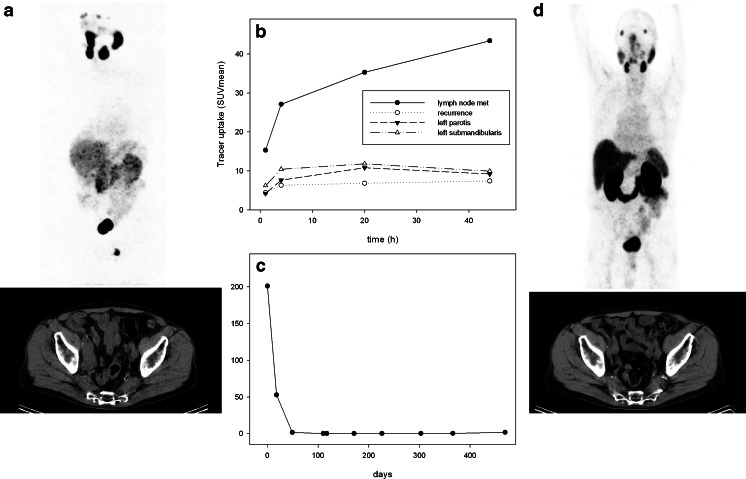
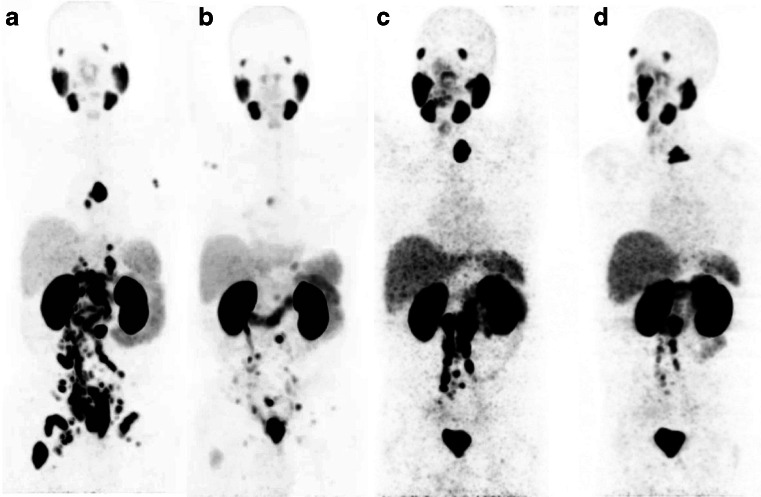
Results: I-124-MIP-1095 PET/CT images showed excellent tumor uptake and moderate uptake in liver, proximal intestine and within a few hours post-injection also in the kidneys. High uptake values were observed only in salivary and lacrimal glands. Dosimetry estimates for I-131-MIP-1095 revealed that the highest absorbed doses were delivered to the salivary glands (3.8 mSv/MBq, liver (1.7 mSv/MBq) and kidneys (1.4 mSv/MBq). The absorbed dose calculated for the red marrow was 0.37 mSv/MBq. PSA values decreased by >50 % in 60.7 % of the men treated. Of men with bone pain, 84.6 % showed complete or moderate reduction in pain. Hematological toxicities were mild. Of men treated, 25 % had a transient slight to moderate dry mouth. No adverse effects on renal function were observed.
Conclusion: Based on the biodistribution and dose calculations of the PSMA-targeted small molecule (124)I-MIP-1095 therapy with the authentic analog (131)I-MIP-1095 enables a targeted tumor therapy with unprecedented doses delivered to the tumor lesions. Involved lymph node and bone metastases were exposed to estimated absorbed doses upwards of 300 Gy.
Figures


References
-
- American Cancer Society, Inc., Surveillance Research; Cancer Facts & Figures, 2012.
-
- National Cancer Institute, Surveillance Epidemiology and End Results. SEER stat fact sheets: prostate. Available from: http://seer.cancer.gov/statfacts/html/prost.html
-
- Smith-Jones PM, Vallabahajosula S, Goldsmith SJ, Navarro V, Hunter CJ, Bastidas D, et al. In vitro characterization of radiolabeled monoclonal antibodies specific for the extracellular domain of prostate-specific membrane antigen. Cancer Res. 2000;60:5237. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
