

Incident heart failure in relation to vascular disease: insights from the Health, Aging, and Body Composition Study
- PMID: 24578142
- PMCID: PMC4648241
- DOI: 10.1002/ejhf.69
Incident heart failure in relation to vascular disease: insights from the Health, Aging, and Body Composition Study
Abstract
Aims: The contribution of heart failure (HF) unrelated to vascular disease to the overall HF burden in older adults is not well characterized. This was investigated in this study.
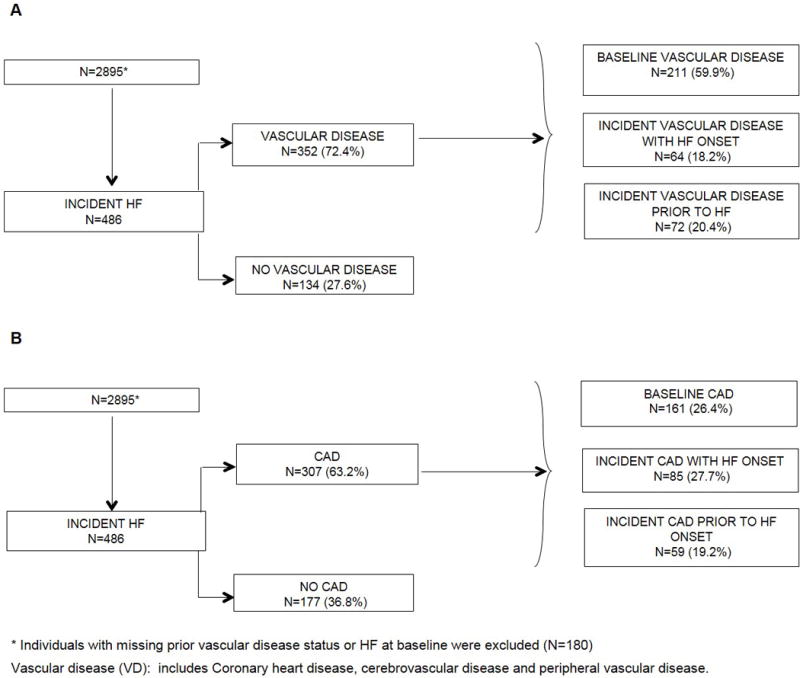
Methods and results: We assessed HF incidence and outcomes in 2895 participants of the Health ABC Study (age 74 ± 3 years, 48.4% men, 41.4% black) in relation to vascular disease (coronary, peripheral, or cerebrovascular disease) either present at baseline or developed prior to HF. During 11.4 years follow-up, 493 participants developed HF; 134 (27.2%) in participants without any prior vascular disease and 177 (36.8%) without coronary disease. Both baseline [hazard ratio (HR) 2.4, 95% confidence interval (CI) 1.9-2.8] and incident vascular disease (HR 4.3, 95% CI 3.6-5.2) were associated with HF. During a median follow-up of 2.1 years after HF onset, 67.5% participants died. Annual mortality after HF development was 21.3% in those with compared with 24.6% in those without vascular disease (HR 1.11, 95% CI 0.87-1.43; P = 0.399). There were 658 all-cause (436.3/1000 person-years) and 523 HF-related (346.4/1000 person-years) hospitalizations after HF development. There was no significant difference in hospitalizations between those with and without vascular disease [rate ratio (RR) 1.04, 95% CI 0.86-1.24 for all-cause, and RR 0.84 95% CI 0.69-1.02 for HF hospitalization]. HF with preserved EF was more common in participants without vascular disease (67.0% vs. 55.0%, P = 0.040).
Conclusion: A significant proportion of HF in older adults develops without prior vascular disease. Outcomes for these patients are poor compared with those with preceding vascular disease. These data suggest the need for more targeted HF prediction and prevention efforts.
Keywords: Epidemiology; Heart failure; Race; Sex.
© 2014 The Authors. European Journal of Heart Failure © 2014 European Society of Cardiology.
Conflict of interest statement
Figures



References
-
- Levy D, Kenchaiah S, Larson MG, Benjamin EJ, Kupka MJ, Ho KKL, Murabito JM, Vasan RS. Long-term trends in the incidence of and survival with heart failure. The New England journal of medicine. 2002;347:1397–1402. - PubMed
-
- Schaufelberger M, Swedberg K, Köster M, Rosén M, Rosengren A. Decreasing one-year mortality and hospitalization rates for heart failure in Sweden; Data from the Swedish Hospital Discharge Registry 1988 to 2000. European heart journal. 2004;25:300–307. - PubMed
-
- Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R, Domanski M, Troutman C, Anderson J, Johnson G, McNulty SE, Clapp-Channing N, Davidson-Ray LD, Fraulo ES, Fishbein DP, Luceri RM, Ip JH. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. The New England journal of medicine. 2005;352:225–237. - PubMed
-
- Cohn JN, Archibald DG, Ziesche S, Franciosa JA, Harston WE, Tristani FE, Dunkman WB, Jacobs W, Francis GS, Flohr KH. Effect of vasodilator therapy on mortality in chronic congestive heart failure. Results of a Veterans Administration Cooperative Study. The New England journal of medicine. 1986;314:1547–1552. - PubMed
-
- Cohn JN, Goldstein SO, Greenberg BH, Lorell BH, Bourge RC, Jaski BE, Gottlieb SO, McGrew F, 3rd, DeMets DL, White BG. A dose-dependent increase in mortality with vesnarinone among patients with severe heart failure. Vesnarinone Trial Investigators. The New England journal of medicine. 1998;339:1810–1816. - PubMed
Publication types
MeSH terms
Grants and funding
- P30 AG024827/AG/NIA NIH HHS/United States
- R01-AG028050/AG/NIA NIH HHS/United States
- N01 AG062101/AG/NIA NIH HHS/United States
- N01-AG-6-2103/AG/NIA NIH HHS/United States
- R01-NR012459/NR/NINR NIH HHS/United States
- R01 NR012459/NR/NINR NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- R01 AG028050/AG/NIA NIH HHS/United States
- N01-AG-6-2106/AG/NIA NIH HHS/United States
- U10 HL110302/HL/NHLBI NIH HHS/United States
- N01-AG-6-2101/AG/NIA NIH HHS/United States
- UL1TR000454/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
