

Monitoring training status with HR measures: do all roads lead to Rome?
- PMID: 24578692
- PMCID: PMC3936188
- DOI: 10.3389/fphys.2014.00073
Monitoring training status with HR measures: do all roads lead to Rome?
Abstract
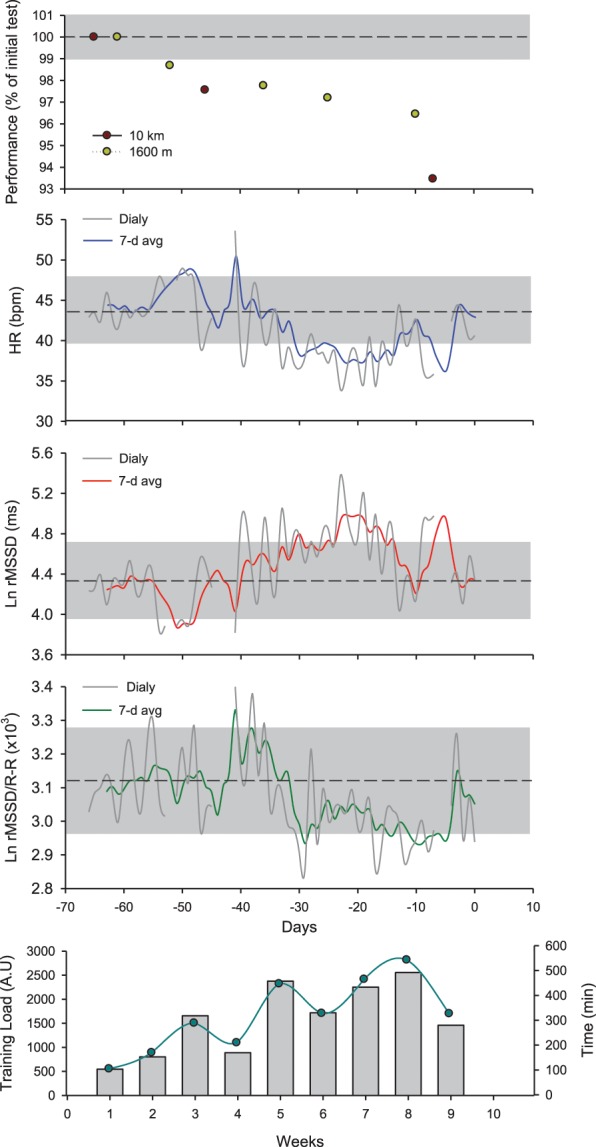
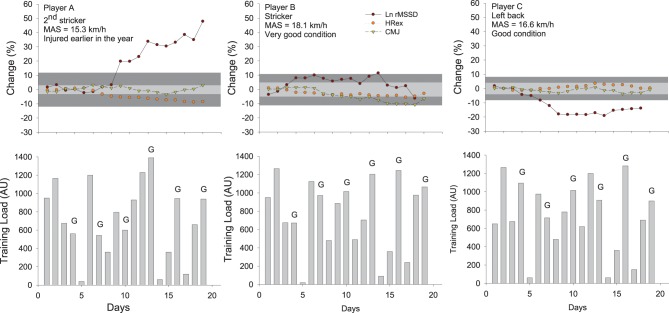
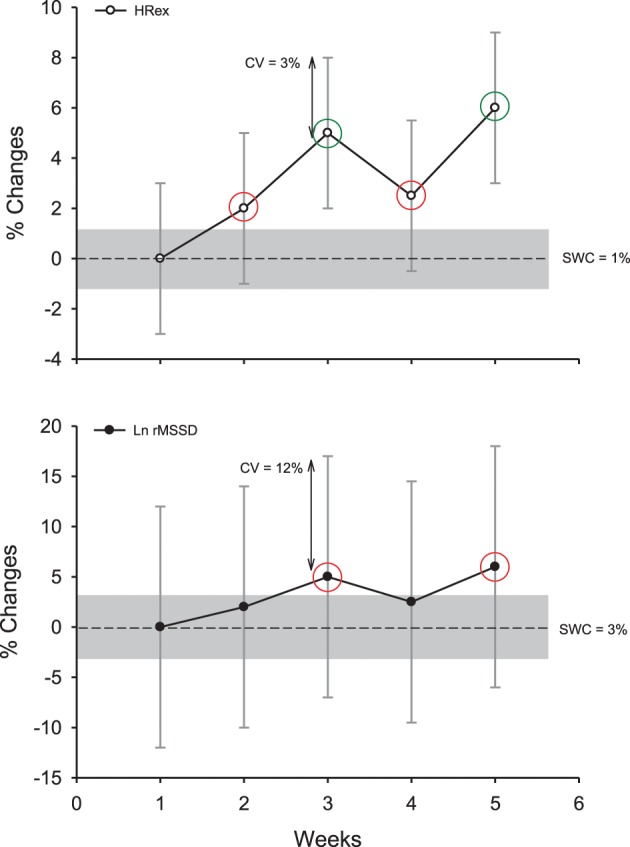
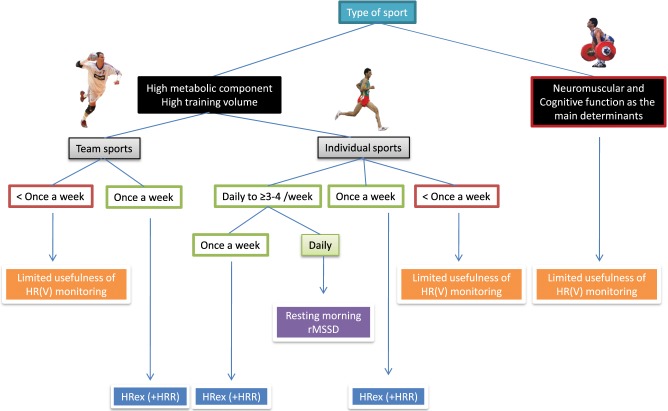
Measures of resting, exercise, and recovery heart rate are receiving increasing interest for monitoring fatigue, fitness and endurance performance responses, which has direct implications for adjusting training load (1) daily during specific training blocks and (2) throughout the competitive season. However, these measures are still not widely implemented to monitor athletes' responses to training load, probably because of apparent contradictory findings in the literature. In this review I contend that most of the contradictory findings are related to methodological inconsistencies and/or misinterpretation of the data rather than to limitations of heart rate measures to accurately inform on training status. I also provide evidence that measures derived from 5-min (almost daily) recordings of resting (indices capturing beat-to-beat changes in heart rate, reflecting cardiac parasympathetic activity) and submaximal exercise (30- to 60-s average) heart rate are likely the most useful monitoring tools. For appropriate interpretation at the individual level, changes in a given measure should be interpreted by taking into account the error of measurement and the smallest important change of the measure, as well as the training context (training phase, load, and intensity distribution). The decision to use a given measure should be based upon the level of information that is required by the athlete, the marker's sensitivity to changes in training status and the practical constrains required for the measurements. However, measures of heart rate cannot inform on all aspects of wellness, fatigue, and performance, so their use in combination with daily training logs, psychometric questionnaires and non-invasive, cost-effective performance tests such as a countermovement jump may offer a complete solution to monitor training status in athletes participating in aerobic-oriented sports.
Keywords: assessing changes; endurance sports; fatigue; heart rate recovery; heart rate variability; progressive statistics; team sports; training response.
Figures
References
-
- Al Haddad H., Parouty J., Buchheit M. (2012). Effect of daily CWI on HRV and subjective ratings of well-being in highly trained swimmers. Int. J. Sports Physiol. Perform. 7, 33–38 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources