

Preoperative prediction of type 2 diabetes remission after Roux-en-Y gastric bypass surgery: a retrospective cohort study
- PMID: 24579062
- PMCID: PMC3932625
- DOI: 10.1016/S2213-8587(13)70070-6
Preoperative prediction of type 2 diabetes remission after Roux-en-Y gastric bypass surgery: a retrospective cohort study
Abstract
Background: About 60% of patients with type 2 diabetes achieve remission after Roux-en-Y gastric bypass (RYGB) surgery. No accurate method is available to preoperatively predict the probability of remission. Our goal was to develop a way to predict probability of diabetes remission after RYGB surgery on the basis of preoperative clinical criteria.
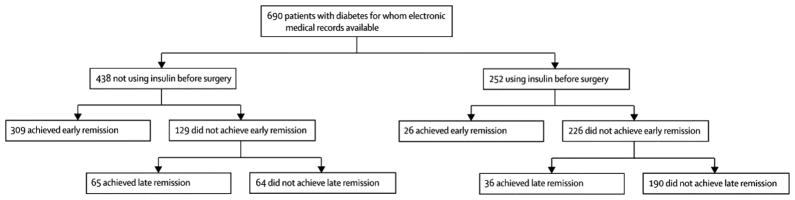
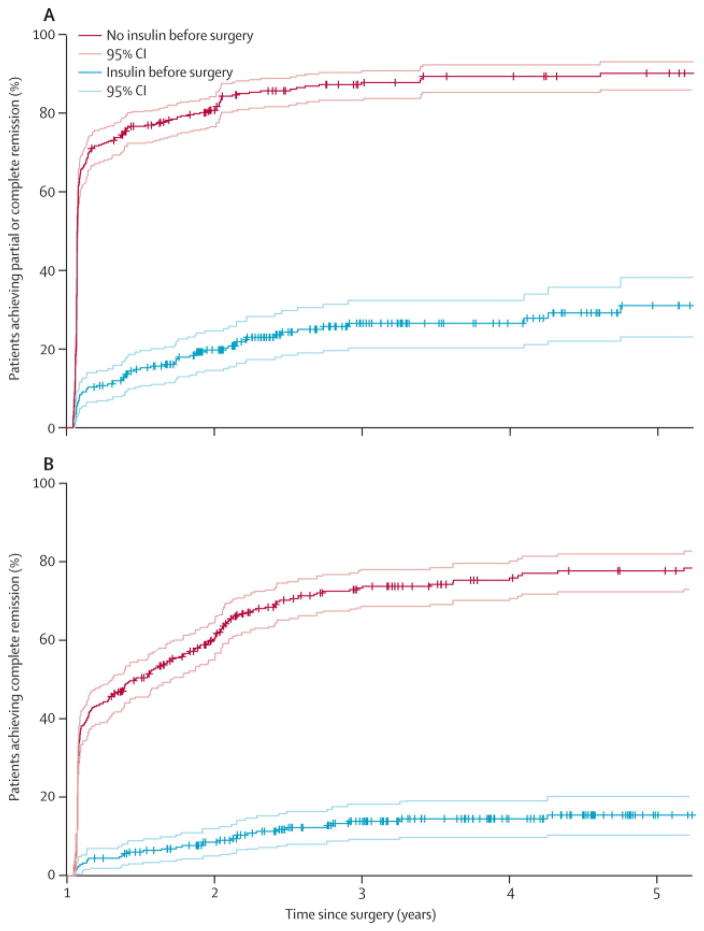
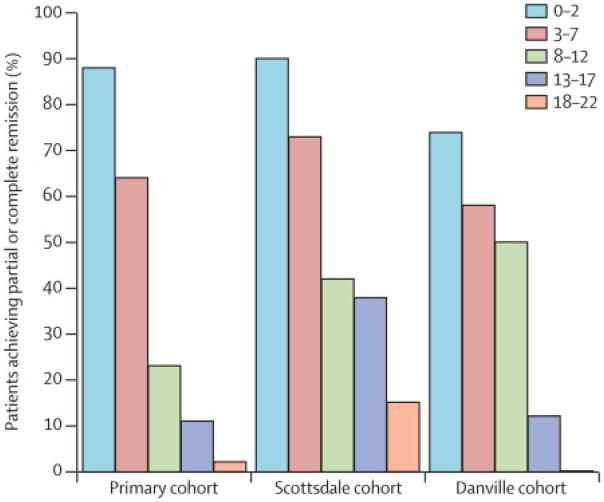
Methods: In a retrospective cohort study, we identified individuals with type 2 diabetes for whom electronic medical records were available from a primary cohort of 2300 patients who underwent RYGB surgery at the Geisinger Health System (Danville, PA, USA) between Jan 1, 2004, and Feb 15, 2011. Partial and complete remission were defined according to the American Diabetes Association criteria. We examined 259 clinical variables for our algorithm and used multiple logistic regression models to identify independent predictors of early remission (beginning within first 2 months after surgery and lasting at least 12 months) or late remission (beginning more than 2 months after surgery and lasting at least 12 months). We assessed a final Cox regression model with a consistent subset of variables that predicted remission, and used the resulting hazard ratios (HRs) to guide creation of a weighting system to produce a score (DiaRem) to predict probability of diabetes remission within 5 years. We assessed the validity of the DiaRem score with data from two additional cohorts.
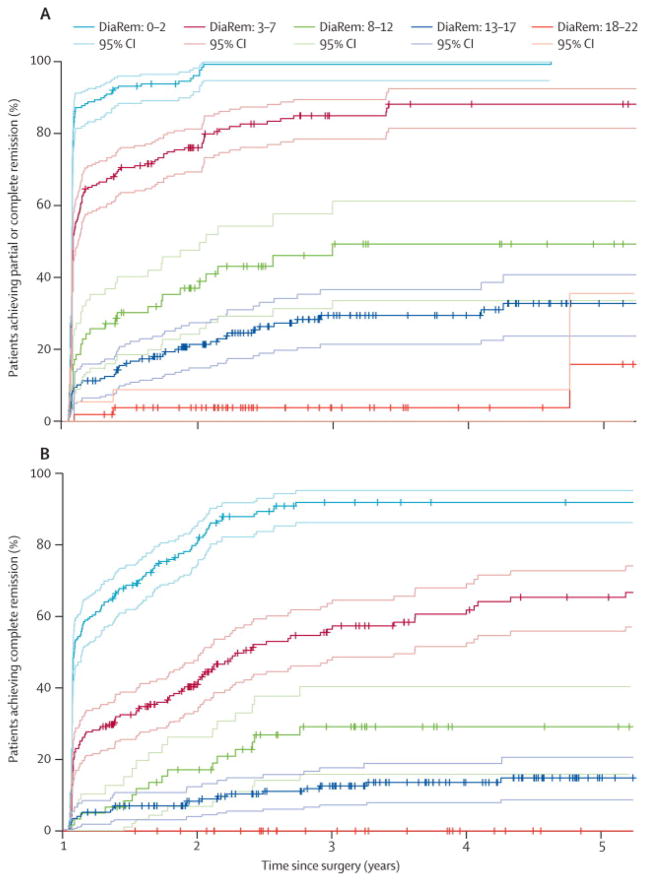
Findings: Electronic medical records were available for 690 patients in the primary cohort, of whom 463 (63%) had achieved partial or complete remission. Four preoperative clinical variables were included in the final Cox regression model: insulin use, age, HbA1c concentration, and type of antidiabetic drugs. We developed a DiaRem score that ranges from 0 to 22, with the greatest weight given to insulin use before surgery (adding ten to the score; HR 5·90, 95% CI 4·41–7·90; p<0·0001). Kaplan-Meier analysis showed that 88% (95% CI 83–92%) of patients who scored 0–2, 64% (58–71%) of those who scored 3–7, 23% (13–33%) of those who scored 8–12, 11% (6–16%) of those who scored 13–17, and 2% (0–5%) of those who scored 18–22 achieved early remission (partial or complete). As in the primary cohort, the proportion of patients achieving remission in the replication cohorts was highest for the lowest scores, and lowest for the highest scores.
Interpretation: The DiaRem score is a novel preoperative method to predict the probability of remission of type 2 diabetes after RYGB surgery.
Funding: Geisinger Health System and the US National Institutes of Health.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Comment in
-
Can we predict diabetes remission after weight-loss surgery?Lancet Diabetes Endocrinol. 2014 Jan;2(1):4-6. doi: 10.1016/S2213-8587(13)70108-6. Epub 2013 Sep 13. Lancet Diabetes Endocrinol. 2014. PMID: 24622655 No abstract available.
-
DiaRem score: external validation.Lancet Diabetes Endocrinol. 2014 Jan;2(1):12-3. doi: 10.1016/S2213-8587(13)70202-X. Epub 2013 Dec 12. Lancet Diabetes Endocrinol. 2014. PMID: 24622660 No abstract available.
-
DiaRem score: external validation--authors' reply.Lancet Diabetes Endocrinol. 2014 Jan;2(1):13. doi: 10.1016/S2213-8587(13)70201-8. Epub 2013 Dec 12. Lancet Diabetes Endocrinol. 2014. PMID: 24622661 Free PMC article. No abstract available.
References
-
- Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes care. 2004;27(5):1047–53. - PubMed
-
- Gill RS, Sharma AM, Al-Adra DP, Birch DW, Karmali S. The impact of bariatric surgery in patients with type-2 diabetes mellitus. Current diabetes reviews. 2001;7(3):185–9. - PubMed
-
- Mingrone G, Panunzi S, De Gaetano A, et al. Bariatric surgery versus conventional medical therapy for type 2 diabetes. N Engl J Med. 2012;366(17):1577–85. - PubMed
-
- Blackstone R, Bunt JC, Cortes MC, Sugerman HJ. Type 2 diabetes after gastric bypass: remission in five models using HbA1c, fasting blood glucose, and medication status. Surgery for obesity and related diseases: official journal of the American Society for Bariatric Surgery. 2012;8(5):548–55. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials