

Therapy duration and long-term outcomes in extra-pulmonary tuberculosis
- PMID: 24580808
- PMCID: PMC3943436
- DOI: 10.1186/1471-2334-14-115
Therapy duration and long-term outcomes in extra-pulmonary tuberculosis
Abstract
Background: Tuberculosis is classified as either pulmonary or extra-pulmonary (EPTB). While much focus has been paid to pulmonary tuberculosis, EPTB has received scant attention. Moreover, EPTB is viewed as one wastebasket diagnosis, as "the other" which is not pulmonary.
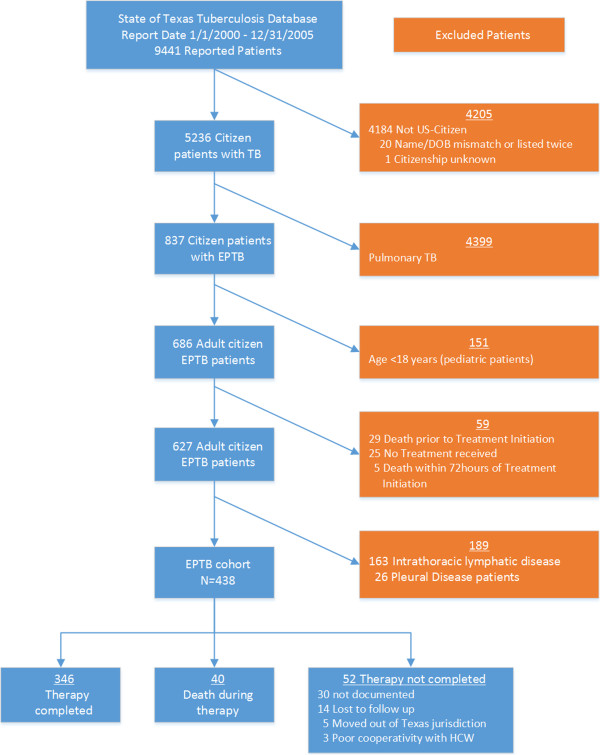
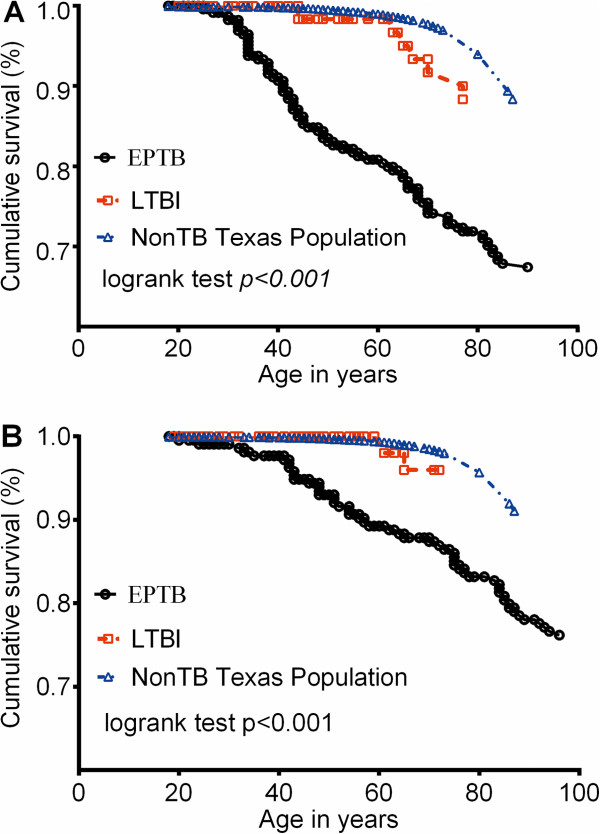
Methods: This is a retrospective cohort study of all patients treated for EPTB in the state of Texas between January 2000 and December 2005, who had no pulmonary disease. Clinical and epidemiological factors were abstracted from electronic records of the Report of Verified Case of Tuberculosis. The long-term outcome, which is death by December 2011, was established using the Social Security Administration Death Master File database. Survival in EPTB patients was compared to those with latent tuberculosis, as well as between different types of EPTB, using Cox proportional hazard models. A hybrid of the machine learning method of classification and regression tree analyses and standard regression models was used to identify high-order interactions and clinical factors predictive of long-term all-cause mortality.
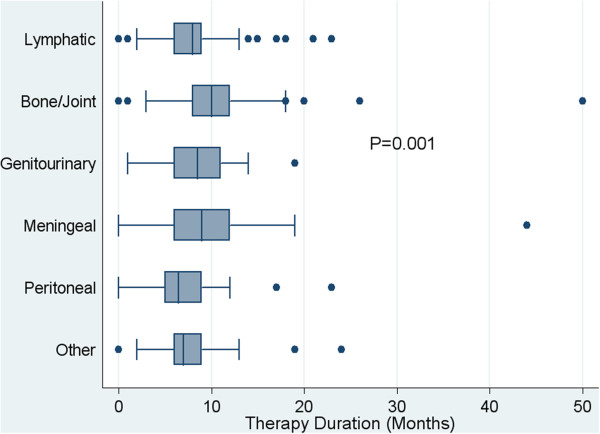
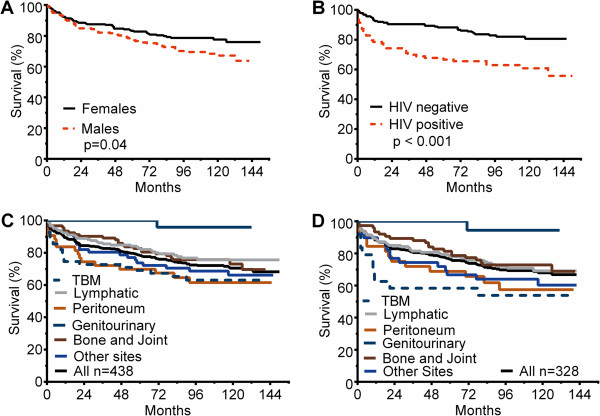
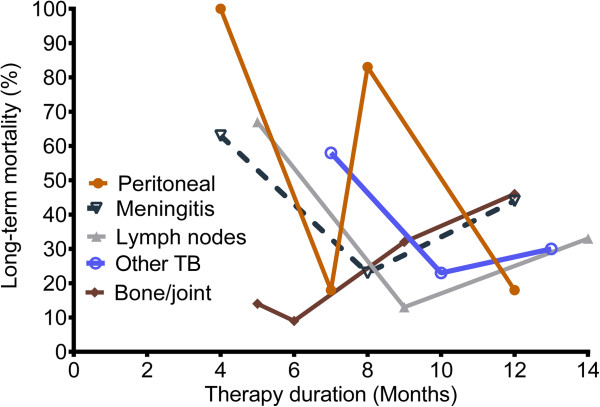
Results: Four hundred and thirty eight patients met study criteria; the median study follow-up period for the cohort was 7.8 (inter-quartile range 6.0-10.1) years. The overall all-cause mortality rate was 0.025 (95% confidence interval [CI]: 0.021-0.030) per 100 person-year of follow-up. The significant predictors of poor long-term outcome were age (hazard ratio [HR] for each year of age-at-diagnosis was 1.05 [CI: 1.04-1.06], treatment duration, type of EPTB and HIV-infection (HR = 2.16; CI: 1.22, 3.83). Mortality in genitourinary tuberculosis was no different from latent tuberculosis, while meningitis had the poorest long-term outcome of 46.2%. Compared to meningitis the HR for death was 0.50 (CI: 0.27-0.91) for lymphatic disease, 0.42 (CI: 0.21-0.81) for bone/joint disease, and 0.59 (CI: 0.27-1.31) for peritonitis. The relationship between mortality and therapy duration for each type of EPTB was a unique "V" shaped curve, with the lowest mortality observed at different therapy durations for each, beyond which mortality increased.
Conclusions: EPTB is comprised of several different diseases with different outcomes and durations of therapy. The "V" shaped relationship between therapy duration and outcome leads to the hypothesis that longer duration of therapy may lead to higher patient mortality.
Figures
References
-
- World Health Organization. Tuberculosis factsheet No 104. Geneva, Switzerland: World Health Organization; 2011.
-
- World Health Organization. TB Epidemiology and Surveillance Workshop. (Increasing/Decreasing Over/Under/Diagnosis of Extrapulmonary TB) Geneva, Switzerland; 2005.
-
- Zhang X, Andersen AB, Lillebaek T, Kamper-Jorgensen Z, Thomsen VO, Ladefoged K, Marrs CF, Zhang L, Yang Z. Effect of sex, age, and race on the clinical presentation of tuberculosis: a 15-year population-based study. Am J Trop Med Hyg. 2011;14:285–290. doi: 10.4269/ajtmh.2011.10-0630. - DOI - PMC - PubMed
-
- Blumberg HM, Burman WJ, Chaisson RE, Daley CL, Etkind SC, Friedman LN, Fujiwara P, Grzemska M, Hopewell PC, Iseman MD, Jasmer RM, Koppaka V, Menzies RI, O’Brien RJ, Reves RR, Reichman LB, Simone PM, Starke JR, Vernon AA. American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America: treatment of tuberculosis. Am J Respir Crit Care Med. 2003;14:603–662. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
