

Congenital anomalous/aberrant systemic artery to pulmonary venous fistula: closure with vascular plugs & coil embolization
- PMID: 24581104
- PMCID: PMC4054825
- DOI: 10.1016/j.ihj.2013.10.009
Congenital anomalous/aberrant systemic artery to pulmonary venous fistula: closure with vascular plugs & coil embolization
Abstract
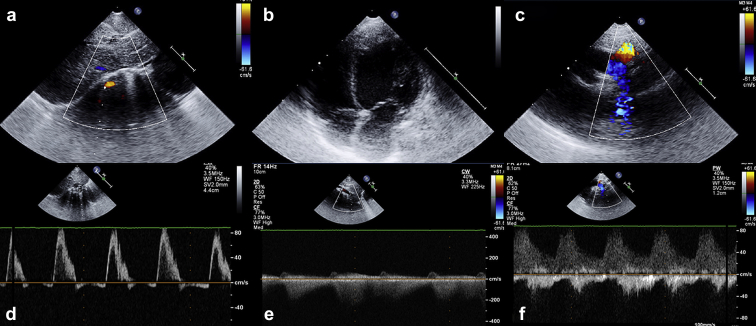
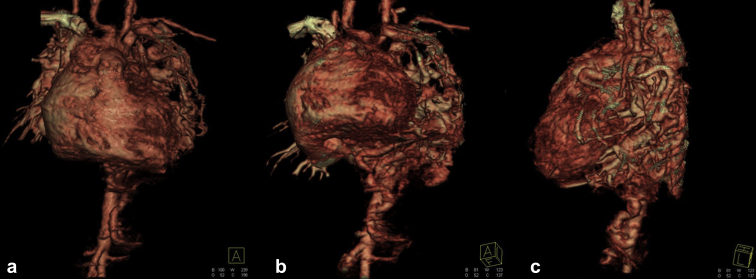
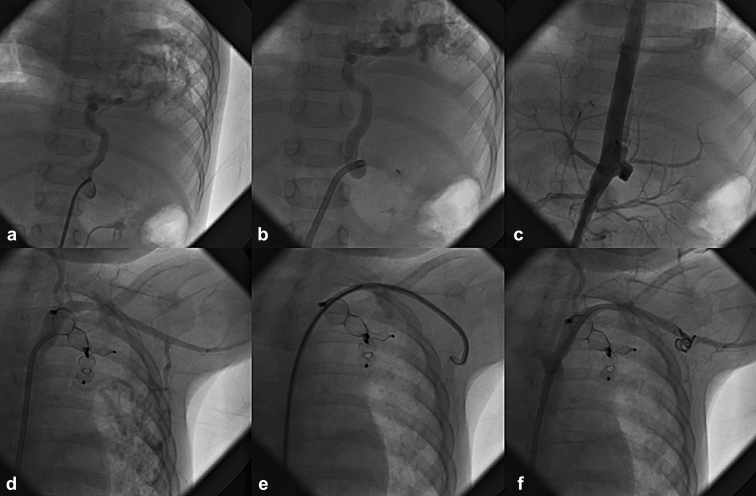
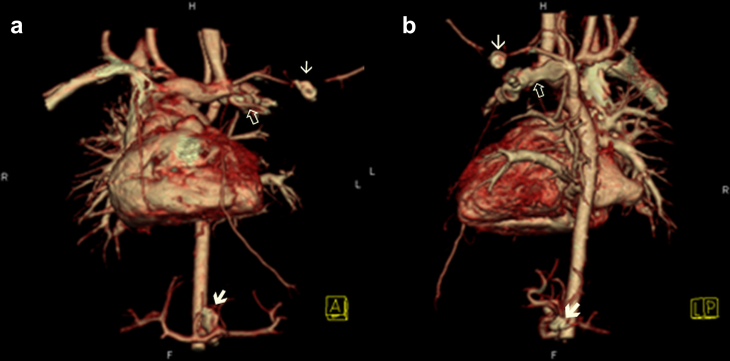
A 7-month-old girl with failure to thrive, who, on clinical and diagnostic evaluation [echocardiography & CT angiography] to rule out congenital heart disease, revealed a rare vascular anomaly called systemic artery to pulmonary venous fistula. In our case, there was dual abnormal supply to the entire left lung as(1) anomalous supply by normal systemic artery [internal mammary artery](2) and an aberrant feeder vessel from the abdominal aorta. Left Lung had normal bronchial connections and normal pulmonary vasculature. The fistula drained through the pulmonary veins to the left atrium leading to 'left-left shunt'. Percutaneous intervention in two stages was performed using Amplatzer vascular plugs and coil embolization to close them successfully. The patient gained significant weight in follow up with other normal developmental and mental milestones.
Keywords: Congenital AV fistula; Sequestration of lung.
Copyright © 2013 Cardiological Society of India. Published by Elsevier B.V. All rights reserved.
Figures


Similar articles
-
Early experience on peripheral vascular application of the vascular plugs.Indian Heart J. 2013 Sep-Oct;65(5):536-45. doi: 10.1016/j.ihj.2013.08.016. Epub 2013 Sep 5. Indian Heart J. 2013. PMID: 24206877 Free PMC article.
-
Arteriovenous fistula between descending aorta and left inferior pulmonary vein: Closure with vascular plugs.Turk Kardiyol Dern Ars. 2016 Mar;44(2):151-3. doi: 10.5543/tkda.2015.28235. Turk Kardiyol Dern Ars. 2016. PMID: 27111314
-
Percutaneous embolization of a caroticoazygous fistula with the Amplatzer Vascular Plug 1.Diagn Interv Radiol. 2012 Jul-Aug;18(4):431-4. doi: 10.4261/1305-3825.DIR.4944-11.2. Epub 2012 Jan 3. Diagn Interv Radiol. 2012. PMID: 22215525
-
Pulmonary arteriovenous malformation.Postgrad Med J. 2002 Apr;78(918):191-7. doi: 10.1136/pmj.78.918.191. Postgrad Med J. 2002. PMID: 11930021 Free PMC article. Review.
-
Development of superior vena cava to pulmonary vein fistulae following modified Fontan operation: case report of a rare anomaly and embolization therapy.Pediatr Cardiol. 1998 Jul-Aug;19(4):363-5. doi: 10.1007/s002469900325. Pediatr Cardiol. 1998. PMID: 9636265 Review.
Cited by
-
Successful percutaneous intervention in a rare case of aberrant systemic artery to a normal lung presented with hemoptysis.J Cardiol Cases. 2021 Mar 7;24(3):122-125. doi: 10.1016/j.jccase.2021.02.011. eCollection 2021 Sep. J Cardiol Cases. 2021. PMID: 34466175 Free PMC article.
-
Left pulmonary sequestration with portal venous drainage: a case description of surgical planning using IQQA-3D reconstruction.Quant Imaging Med Surg. 2025 Jun 6;15(6):5893-5899. doi: 10.21037/qims-2024-2694. Epub 2025 May 26. Quant Imaging Med Surg. 2025. PMID: 40606364 Free PMC article. No abstract available.
-
A rare case of congenital anomalous/aberrant systemic artery to pulmonary venous fistula in a 4-month-old child with co-existent mitral valve prolapse and mitral regurgitation.BMJ Case Rep. 2015 Sep 21;2015:bcr2015210865. doi: 10.1136/bcr-2015-210865. BMJ Case Rep. 2015. PMID: 26392446 Free PMC article. No abstract available.
-
Isolated arterial pulmonary malinosculation without sequestration in an adult: A case report and literature review.Respir Med Case Rep. 2021 Sep 10;34:101514. doi: 10.1016/j.rmcr.2021.101514. eCollection 2021. Respir Med Case Rep. 2021. PMID: 34540582 Free PMC article.
-
Decision changing in the operating room: The importance of the surgeon's certainty and a well prepared team.Lung India. 2016 Sep-Oct;33(5):556-7. doi: 10.4103/0970-2113.188984. Lung India. 2016. PMID: 27625456 Free PMC article. No abstract available.
References
-
- Wong M.N.L., Joshi P., Sim K.H. Large anomalous systemic arterial supply to the left lung without pulmonary sequestration: a rare cause of heart failure in a child. Pediatr Cardiol. 2009 Jan;30:85–86. - PubMed
-
- Varma K.K., Clarke C.P. Congenital systemic-to-pulmonary arteriovenous fistula: report of a case. Aust N Z J Surg. 1971 May;40:360–362. - PubMed
-
- Geyik S., Yavuz K., Keller F.S. Unusual systemic artery to pulmonary artery malformation without evidence of systemic disease, trauma or surgery. Cardiovasc Intervent Radiol. 2006;29:897–901. - PubMed
-
- Pryce D.M., Sellors T.H., Blair L.G. Intralobar sequestration of lung associated with an abnormal artery. Br J Surg. 1947;35:18–29. - PubMed
-
- Albertini A., Dell'Amore A., Tripodi A. Anomalous systemic arterial supply to the left lung base without sequestration. Heart Lung Circ. 2008 Dec;17:505–507. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
