

Diverse arachnoid cyst morphology indicates different pathophysiological origins
- PMID: 24581284
- PMCID: PMC4078003
- DOI: 10.1186/2045-8118-11-5
Diverse arachnoid cyst morphology indicates different pathophysiological origins
Abstract
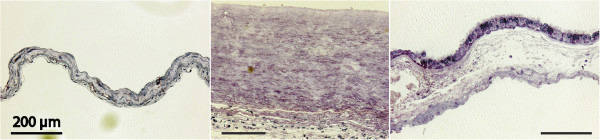
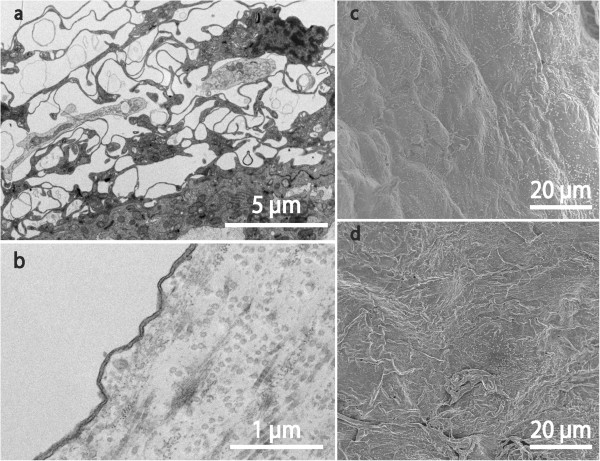
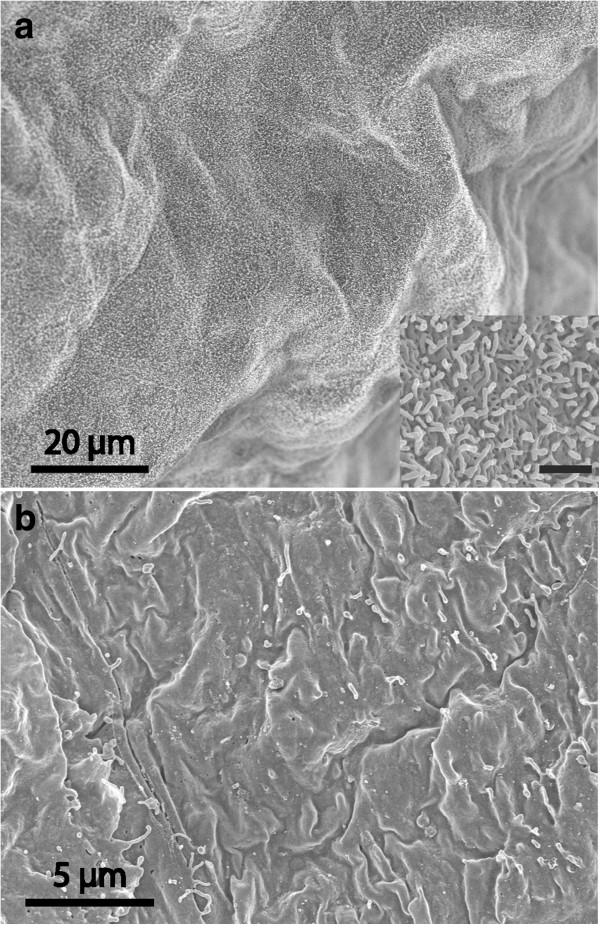
Background: There are few, limited, and to some extent contradictory, reports on the cellular and subcellular morphology of arachnoid cysts. In the literature cyst membranes are described as similar to, or as vastly different from, normal arachnoid membranes.
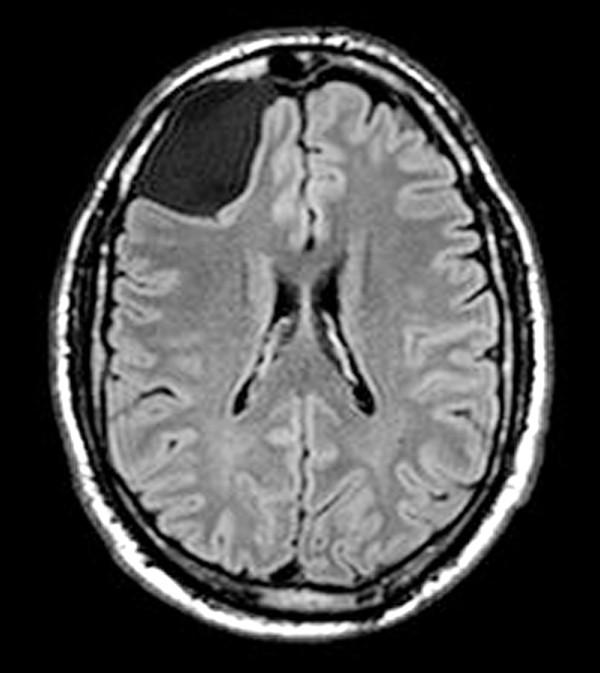
Methods: This paper reports electron microscopic analyses of symptomatic cysts from 24 patients (12 males and 12 females; age 10-79), that underwent fenestration surgery. Fourteen cysts were located in the middle cranial fossa (temporal), one in the interpeduncular cistern, five in the posterior fossa, and four were overlying the frontal cortex.
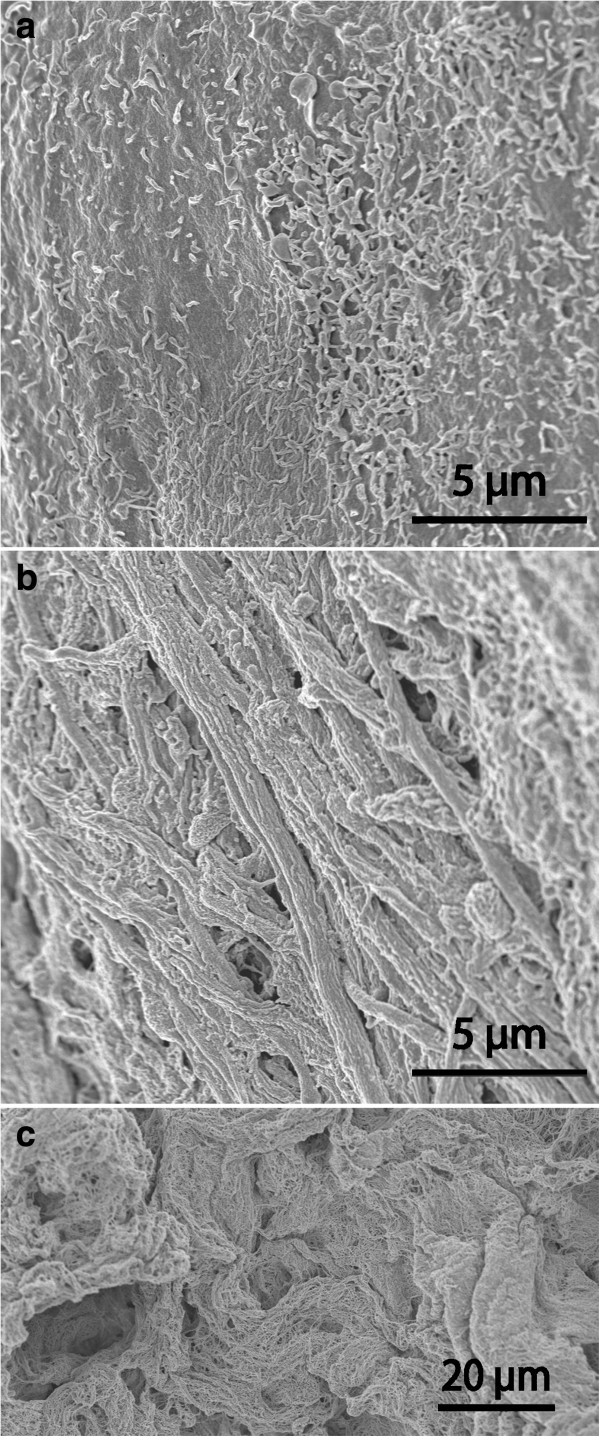
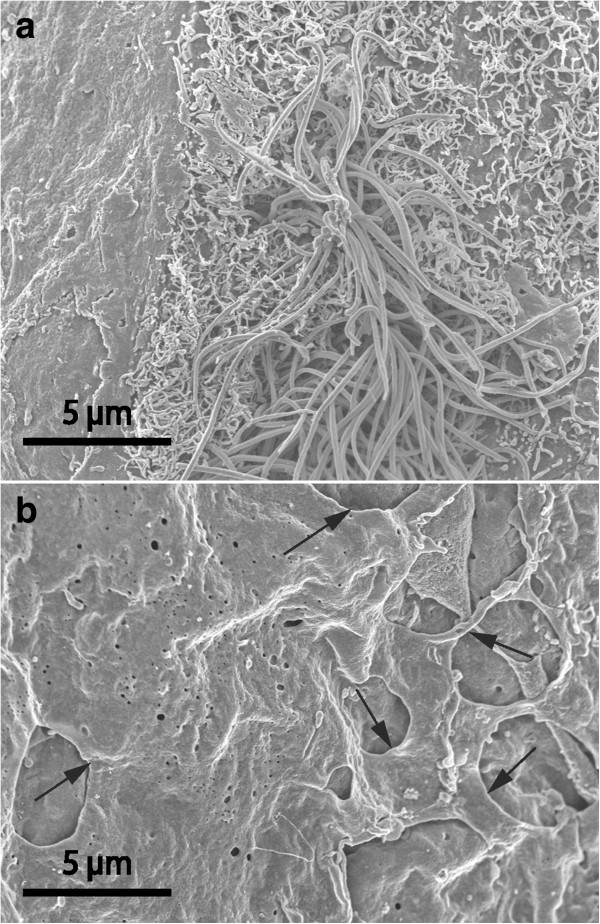
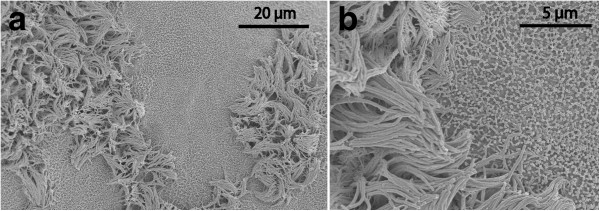
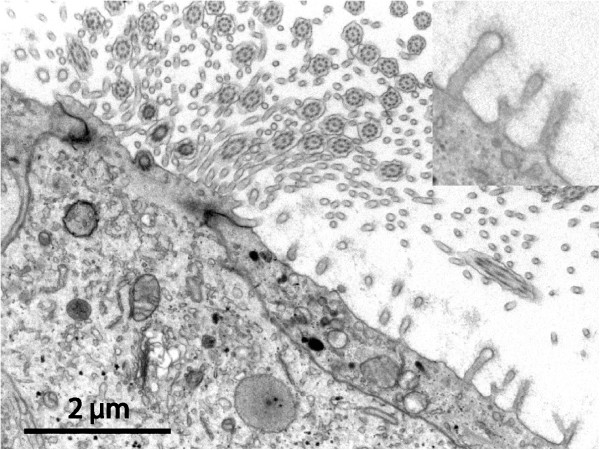
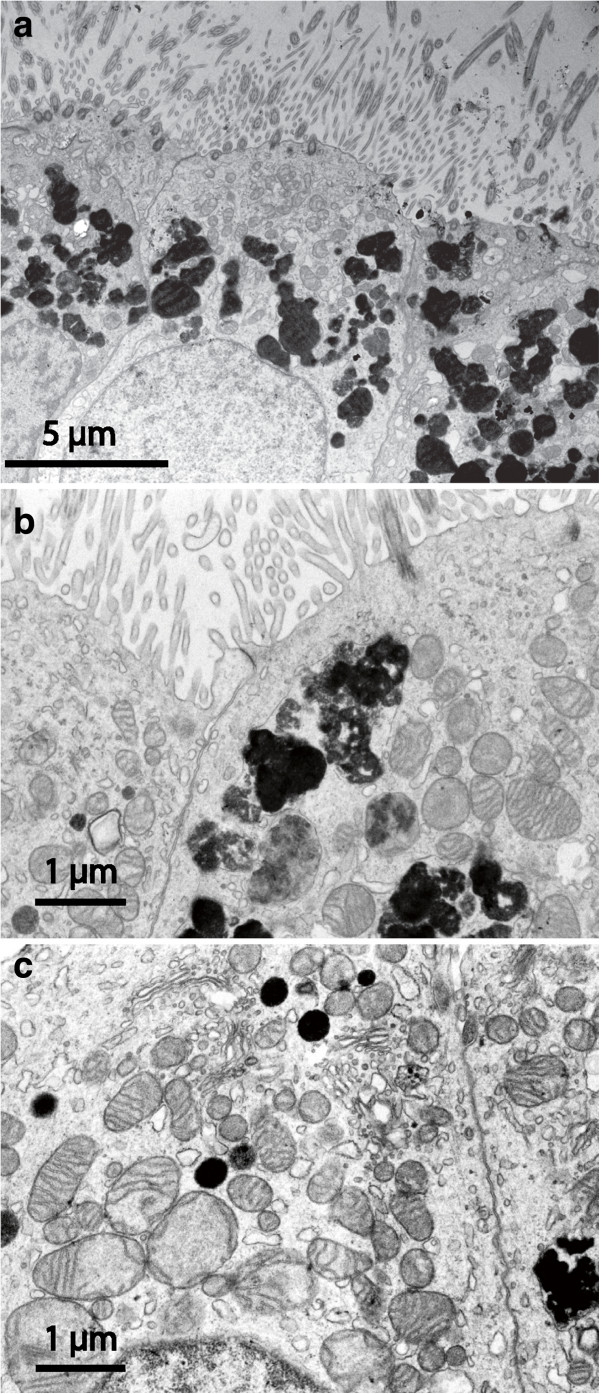
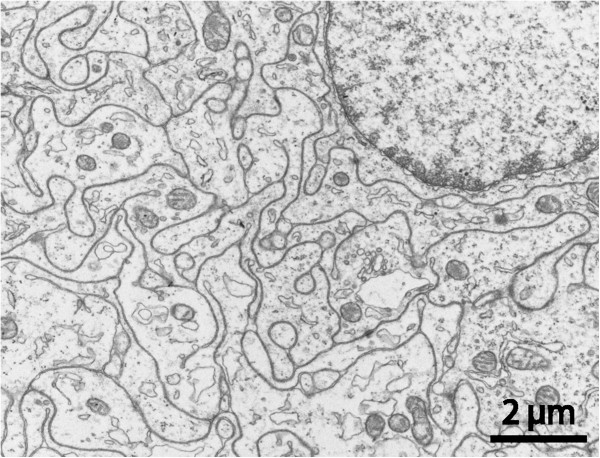
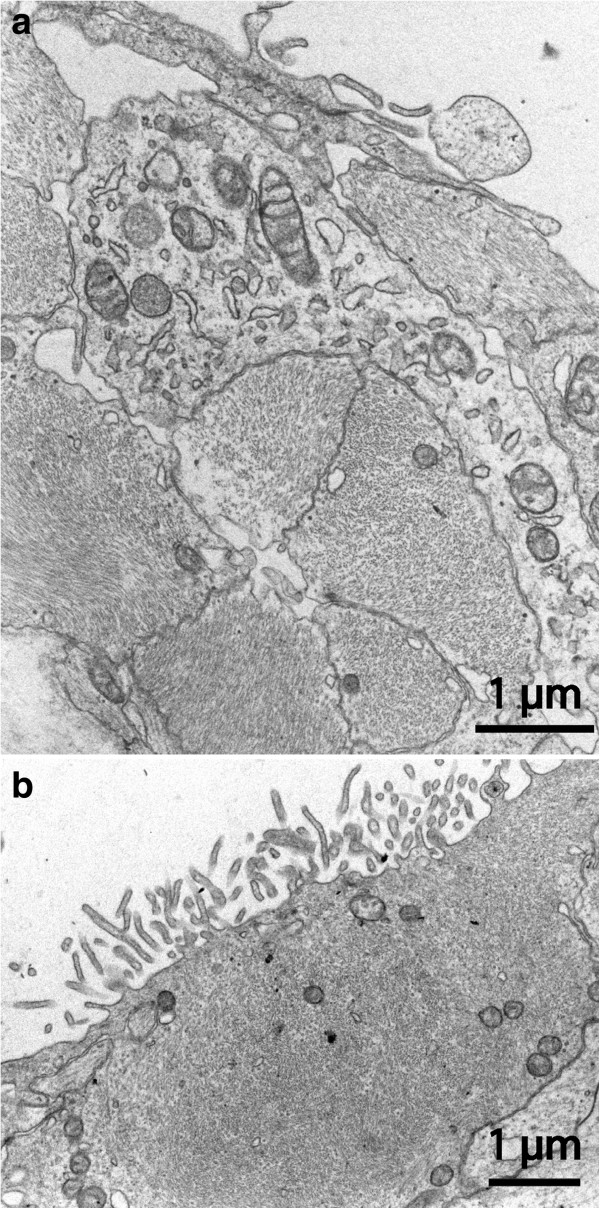
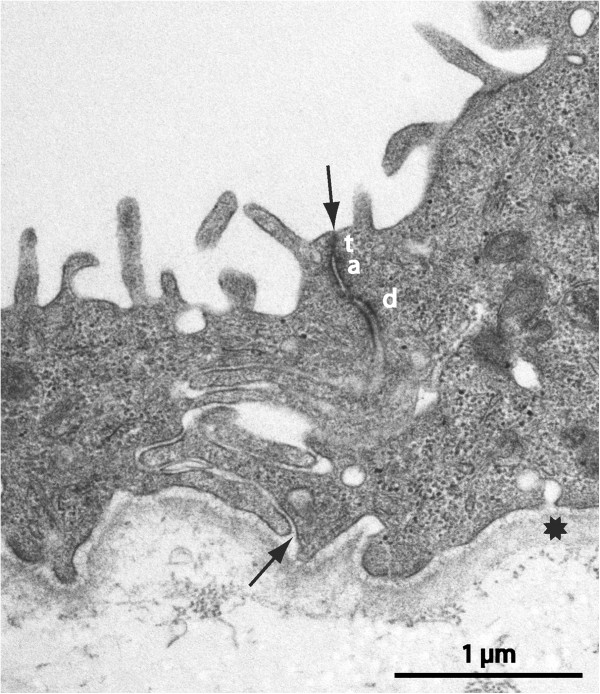
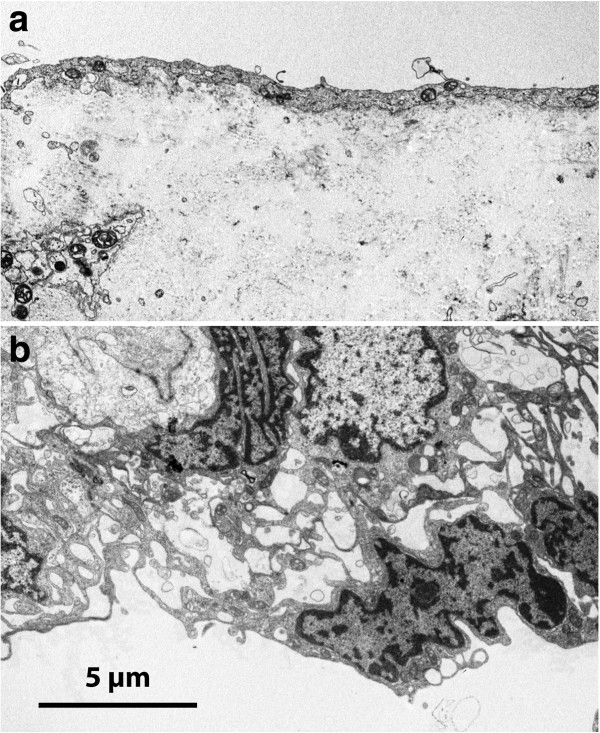
Results: Microscopic findings confirmed the diverse nature of this clinical condition. Twelve cyst walls resembled normal arachnoid, four had a conspicuous core of dense fibrous tissue with a simple epithelial lining, and the remaining aberrant cysts exhibited non-arachnoid luminal epithelia with plentiful microvilli and/or cilia, and also nervous tissue components in the wall. The possible identity and origin of various cyst types are discussed. We hypothesize that cysts are formed mostly at an early stage of embryonic development, as a teratological event.
Conclusions: Cysts with various epithelial linings and extracellular components most likely have different barrier properties and fluid turnover characteristics. Further studies are needed to elucidate relations between cyst morphology, fluid composition, pathogenesis, and clinical behaviour including growth rate and relapse tendency.
Figures
References
-
- Rengachary SS, Watanabe I, Brackett CE. Pathogenesis of intracranial arachnoid cysts. Surg Neurol. 1978;9:139–144. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
